- Cluster headache
-
Cluster headache Classification and external resources 
The Cluster Headache by JD FletcherICD-10 G44.0 ICD-9 339.00,339.01,339.02, DiseasesDB 2850 eMedicine EMERG/229 NEURO/67 MeSH D003027 Cluster headache, nicknamed "suicide headache", is a neurological disease that involves, as its most prominent feature, an immense degree of pain in the head. Cluster headaches occur periodically: spontaneous remissions interrupt active periods of pain. The cause of the disease is currently unknown. It affects approximately 0.1% of the population, and men are more commonly affected than women.
Contents
Signs and symptoms
Cluster headaches are excruciating unilateral headaches[1] of extreme intensity.[2] The duration of the common attack ranges from as short as 15 minutes to three hours or more. The onset of an attack is rapid, and most often without the preliminary signs that are characteristic of a migraine. However, some sufferers report preliminary sensations of pain in the general area of attack, often referred to as "shadows", that may warn them an attack is lurking or imminent. Though the headaches are almost exclusively unilateral, there are some documented as cases of "side-shifting" between cluster periods, or, even rarer, simultaneously (within the same cluster period) bilateral headache.[3] Trigeminal neuralgia can also bring on headaches with similar qualities. However, with trigeminal neuralgia the pain is mostly located around the facial area and is described as being like stabbing electric shocks, burning, pressing, crushing, exploding or shooting pain that becomes intractable.
Pain
The pain may be very sharp and may cause pain around the eye area and may also be a pain within the back of the eye. The pain of cluster headaches is markedly greater than in other headache conditions, including severe migraines; experts have suggested that it may be the most painful condition known to medical science. Female patients have reported it as being more severe than childbirth.[4] Dr. Peter Goadsby, Professor of Clinical Neurology at University College London (now University of California, San Francisco), a leading researcher on the condition has commented:
"Cluster headache is probably the worst pain that humans experience. I know that’s quite a strong remark to make, but if you ask a cluster headache patient if they’ve had a worse experience, they’ll universally say they haven't. Women with cluster headache will tell you that an attack is worse than giving birth. So you can imagine that these people give birth without anesthetic once or twice a day, for six, eight, or ten weeks at a time, and then have a break. It's just awful."[5]
The pain is lancinating or boring/drilling in quality, and is located behind the eye (periorbital) or in the temple, sometimes radiating to the neck or shoulder. Analogies frequently used to describe the pain are a red-hot poker inserted into the eye, or a spike penetrating from the top of the head, behind one eye, radiating down to the neck, or sometimes having a leg amputated without any anaesthetic. The condition was originally named Horton's Cephalalgia after Dr. B.T Horton, who postulated the first theory as to their pathogenesis. His original paper describes the severity of the headaches as being able to take normal men and force them to attempt or complete suicide. From Horton's 1939 paper on cluster headache:
"Our patients were disabled by the disorder and suffered from bouts of pain from two to twenty times a week. They had found no relief from the usual methods of treatment. Their pain was so severe that several of them had to be constantly watched for fear of suicide. Most of them were willing to submit to any operation which might bring relief."[6]
Thus, cluster headaches are also known by the nickname "suicide headaches".[7]
Other symptoms
The cardinal symptoms of the cluster headache attack are the severe or very severe unilateral orbital, supraorbital and/or temporal pain lasting 15–180 minutes, if untreated, and the attack frequency of one to 16 attacks in 48 hours. The headache is accompanied by at least one of the following autonomic symptoms: ptosis (drooping eyelid), miosis (pupil constriction) conjunctival injection (redness of the conjunctiva), lacrimation (tearing), rhinorrhea (runny nose), and, less commonly, facial blushing, swelling, or sweating, all appearing on the same side of the head as the pain.[8] The attack is also associated with restlessness, the sufferer often pacing the room or rocking back and forth. Less frequently, he or she will have an aversion to bright lights and loud noise during the attack. Nausea rarely accompanies a cluster headache, though it has been reported. The neck is often stiff or tender in the aftermath of a headache, with jaw or tooth pain sometimes present. Some sufferers report feeling as though their nose is stopped up and that they are unable to breathe out of one of their nostrils.
Secondary effects are inability to organize thoughts and plans, exhaustion (in response to such extreme stress, body shuts down and only wants to sleep/repair), and depression. Patients tend to dread facing another headache, and may adjust their physical activities or ask for help to accomplish normal tasks, and may hesitate to schedule plans in reaction to the clock-like regularity of the pain schedule leading to social isolation.
Recurrence
Cluster headaches are occasionally referred to as "alarm clock headaches" because of their ability to wake a person from sleep and because of the regularity of their timing: both the individual attacks and the clusters themselves can have a metronomic regularity; attacks striking at a precise time of day each morning or night is typical, even precisely at the same time a week later. The clusters tend to follow daylight saving time changes and happen more often in spring and fall equinox. This has prompted researchers to speculate an involvement of the brain's "biological clock" or circadian rhythm.
In episodic cluster headaches, these attacks occur once or more daily, often at the same times each day, for a period of several weeks, followed by a headache-free period lasting weeks, months, or years. Approximately 10–15% of cluster headache sufferers are chronic; they can experience multiple headaches every day for years.
Cluster headaches occurring in two or more cluster periods lasting from 7 to 365 days with a pain-free remission of one month or longer between the clusters are considered episodic. If the attacks occur for more than a year without a pain-free remission of at least one month, the condition is considered chronic.[9] Chronic clusters run continuously without any "remission" periods between cycles. The condition may change from chronic to episodic and from episodic to chronic. Remission periods lasting for decades before the resumption of clusters have been known to occur.
Pathophysiology
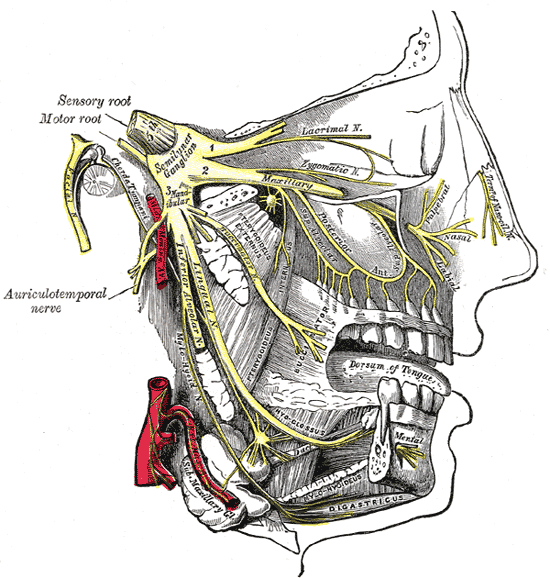
 Gray's FIG. 778– Trigeminal nerve is shown in yellow.
Gray's FIG. 778– Trigeminal nerve is shown in yellow.
 Gray's FIG. 777– Detailed view of ophthalmic nerve, shown in yellow.
Gray's FIG. 777– Detailed view of ophthalmic nerve, shown in yellow.Cluster headaches have been classified as vascular headaches. The intense pain is caused by the dilation of blood vessels which creates pressure on the trigeminal nerve. While this process is the immediate cause of the pain, the etiology (underlying cause or causes) is not fully understood.
Recently, researchers have linked low testosterone as a possible cause of cluster headaches.[10][11]
Hypothalamus
Among the most widely accepted theories is that cluster headaches are due to an abnormality in the hypothalamus; Dr Goadsby, an Australian specialist in the disease has developed this theory. This can explain why cluster headaches frequently strike around the same time each day, and during a particular season, since one of the functions the hypothalamus performs is regulation of the biological clock. Metabolic abnormalities have also been reported in patients.
The hypothalamus is responsive to light—daylength and photoperiod; olfactory stimuli, including sex steroids and corticosteroids; neurally transmitted information arising in particular from the heart, the stomach, and the reproductive system; autonomic inputs; blood-borne stimuli, including leptin, ghrelin, angiotensin, insulin, pituitary hormones, cytokines, blood plasma concentrations of glucose and osmolarity, etc.; and stress. These particular sensitivities may underlay the causes, triggers, and methods of treatment of cluster headache.
Neuroimaging 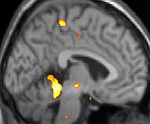
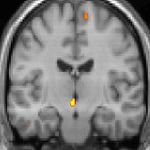

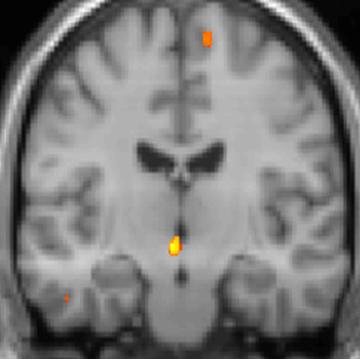
Positron emission tomography (PET) shows brain areas being activated during pain 
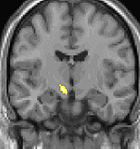
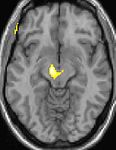
Voxel-based morphometry (VBM) shows brain area structural differences The above Positron emission tomography (PET) pictures indicate the brain areas which are activated during pain only, compared to the pain free periods. These pictures show brain areas which are always active during pain in yellow/orange colour (called "pain matrix"). The area in the centre (in all three views) is specifically activated during cluster headache only. The bottom row Voxel-based morphometry (VBM) pictures show structural brain differences between cluster headache patients and people without headaches; only a portion of the hypothalamus is different.[12][13]
Genetics
There is a genetic component to cluster headaches, although no single gene has been identified as the cause. First-degree relatives of sufferers are more likely to have the condition than the population at large.[14]
Smoking
Tobacco consumption may trigger cluster headaches, and the affliction is often found in people with a heavy addiction to cigarette smoking. In some cases second hand smoke may trigger cluster headaches. However it is not clear if there is a causal relationship between smoking and cluster headaches. Some researchers think that people who suffer from cluster headaches may be predisposed to certain traits, including smoking or other lifestyle habits.[15]
Diagnosis
Cluster headaches often go undiagnosed for many years, being confused with migraine or other causes of headache.[16]
Many times a headache diary is useful- tracking when and where the pain occurs, how severe it is, how long the pain lasts, and coping strategies used will help a physician distinguish between the types of headaches.
Cluster headaches are benign, but because of the extreme and debilitating pain associated with them, and potential risk of suicide, a severe attack is nevertheless treated as a medical emergency. Because of the relative rareness of the condition and ambiguity of the symptoms, some sufferers may not receive treatment in the emergency room and people may even be mistaken as exhibiting drug-seeking behavior.
Differential
There are other types of headache that are sometimes mistaken for cluster headaches.
- Chronic Paroxysmal Hemicrania (CPH) is a condition similar to cluster headache, but CPH responds well to treatment with the anti-inflammatory drug indomethacin and the attacks are much shorter, often lasting only seconds.[17]
- Some people with extreme headaches of this nature (especially if they are not unilateral) may actually have an ictal headache. Anti-convulsant medications can significantly improve this condition so sufferers should consult a physician about this possibility.[18]
Prevention
A wide variety of prophylactic medicines are in use, and patient response to these is highly variable. Current European guidelines suggest the use of the calcium channel blocker verapamil at a dose of at least 240 mg daily. Steroids, such as prednisolone/prednisone, are also effective, with a high dose given for the first five days or longer (in some cases up to 6 months) before tapering down. Methysergide, lithium and the anticonvulsant topiramate are recommended as alternative treatments.[19] In Australia, Neurologist John Watson has also reported success with Epilim and Tegretol in some chronic, treatment-refractory cases.
Intravenous magnesium sulfate relieves cluster headaches in about 40% of patients with low serum ionized magnesium levels.[20] Melatonin has also been demonstrated to bring significant improvement in approximately half of episodic patients.[21]
Management
Main article: Cluster headache treatmentsOver-the-counter pain medications (such as aspirin, paracetamol, and ibuprofen) typically have no effect on the pain from a cluster headache. Unlike other headaches such as migraines and tension headaches, cluster headaches do not respond to biofeedback.[citation needed]
Medications to treat cluster headaches are classified as either abortives or prophylactics (preventatives). In addition, short-term transitional medications (such as steroids) may be used while prophylactic treatment is instituted and adjusted. With abortive treatments often only decreasing the duration of the headache and preventing it from reaching its peak rather than eliminating it entirely, preventive treatment is always indicated for cluster headaches, to be started at the first sign of a new cluster cycle.
Oxygen
During the onset of a cluster headache, many people respond to inhalation of 100% oxygen (12-15 litres per minute in a non-re-breathing mask). Some people have found better results with 25 litres per minute. There is also a study (commenced 2011) using an "on-demand" valve that can deliver up to 160 litres per minute. [1] [19][22][23] When oxygen is used at the onset this can abort the attack in as little as 1 minute or as long as 10 minutes. Once an attack is at its peak, oxygen therapy appears to have little effect so many people keep an oxygen tank close at hand to use at the very first sign of an attack. An alternative first-line treatment is subcutaneous or intranasal administration of sumatriptan.[19] Hyperbaric oxygen therapy has been used successfully in treating cluster headaches though it was not shown to be more successful than surface oxygen.[24][25][26]
Triptans
Sumatriptan and zolmitriptan have both been shown to improve symptoms during an attack.[27]
Other
Some non-narcotic treatments that have shown mixed levels of success are botox injections along the occipital nerve, as well as sarapin (pitcher plant extract) injections.[28][29]
Lidocaine and other topical anesthetics sprayed into the nasal cavity may relieve or stop the pain,[30] normally in a few minutes, but long term use is not suggested due to the side effects and possible damage to the nasal cavities.
Previously, vaso-constrictors such as ergot compounds were also used, and sufferers report a similar relief by taking strong cups of coffee immediately at the onset of an attack. Cafergot, a cheap off-the-shelf vaso-constrictor, has been shown to stop cluster headaches within 40 minutes of ingestion. BOL (2-bromo lysergic acid diethylamide), a non-psychedelic form of the ergot-derived psychedelic LSD, has shown promise in the treatment of cluster headaches.[31]
Kudzu, a common vine from the Pea subfamily Faboideae, may prove to have a role in the management of cluster headache.[32]
Other abortive remedies that work for some include ice, hot showers, cool or lukewarm water sprayed on the face around the sinus, temple, and ear areas, breathing cold air, application of White Flower analgesic balm beneath the nostrils, caffeine, and drinking large amounts of water in the early stages of an attack. Vigorous exercise has been shown in some cases to be very effective in relieving and aborting an acute attack by increasing the levels of oxygen within the body. This could also be due to an increase in adrenaline and changes in blood pressure. Some people report that sexual intercourse and specifically orgasm may terminate an attack possibly by acutely modulating hypothalamic function. Concentrating one's thoughts to a remote part of one's anatomy, such as the opposite little toe, reduced the length of attacks. Headaches are self-perpetuating by concentrating the mind on the symptoms.[33][34][35]
Epidemiology
While migraines are diagnosed more often in women, cluster headaches are more prevalent in men. The male-to-female ratio in cluster headache ranges from 4:1 to 7:1. It primarily occurs between the ages of 20 to 50 years.[36] This gap between the sexes has narrowed over the past few decades, and it is not clear whether cluster headaches are becoming more frequent in women, or whether they are merely being better diagnosed. Limited epidemiological studies have suggested prevalence rates of between 56 and 326 people per 100,000.[37]
History
The first complete description of cluster headache was given by the London neurologist Wilfred Harris in 1926. He named the disease Migrainous neuralgia.[38][39][40]
Cluster headaches have been called by several other names in the past including Erythroprosopalgia of Bing, Ciliary neuralgia, Erythromelagia of the head, Horton's headache (named after Bayard T. Horton, an American neurologist), Histaminic cephalalgia, Petrosal neuralgia, sphenopalatine neuralgia, Vidian neuralgia, Sluder's neuralgia, and Hemicrania angioparalyticia.[41] Sluder's neuralgia (syndrome) and cluster pain can often be temporarily stopped with nasal lidocaine drops.[42][43]
-

Robert Bing (1878–1956)
-

Bayard T. Horton (1895–1980)
See also
- Tension headaches
- Migraine
- Rebound headaches
- Hemicrania continua
- Trigeminal neuralgia
- Chronic Paroxysmal Hemicrania
- Organization for Understanding Cluster Headaches
References
- ^ Beck E, Sieber WJ, Trejo R (February 2005). "Management of cluster headache". Am Fam Physician 71 (4): 717–24. PMID 15742909. http://www.aafp.org/afp/20050215/717.html.
- ^ Capobianco DJ, Dodick DW (April 2006). "Diagnosis and treatment of cluster headache". Semin Neurol 26 (2): 242–59. doi:10.1055/s-2006-939925. PMID 16628535.
- ^ Meyer EL, Laurell K, Artto V, Bendtsen L, Linde M, Kallela M, Tronvik E, Zwart JA, Jensen RM, Hagen K (June 2009). "Lateralization in cluster headache: a Nordic multicenter study". J Headache Pain 10 (4): 259–63. doi:10.1007/s10194-009-0129-z. PMID 19495933. PDF Comment Dr. Andrew Sewell
- ^ Matharu M, Goadsby P (October 2001). "Cluster Headache -- Update on a Common Neurological Problem" (PDF). Practical Neurology 1 (1): 42–9. doi:10.1046/j.1474-7766.2001.00505.x. http://pn.bmj.com/cgi/reprint/1/1/42.
- ^ http://www.abc.net.au/rn/talks/8.30/helthrpt/stories/s42434.htm
- ^ Horton BT, MacLean AR, Craig W.: A New Syndrome of Vascular Headache: Results of Treatment with Histamine. Proc Staff Meet, Mayo Clinic (1939) 14:257
- ^ "Cluster Headaches Can Make Life Unbearable". ABC News. 2001-06-13. http://abcnews.go.com/GMA/PainManagement/story?id=126909. Retrieved 2010-02-05.
- ^ IHS/ICHD-II 3.1 Cluster headache
- ^ IHS Classification ICHD-II 3.1.2 Chronic cluster headache
- ^ Stillman MJ (June 2006). "Testosterone replacement therapy for treatment refractory cluster headache". Headache 46 (6): 925–33. doi:10.1111/j.1526-4610.2006.00436.x. PMID 16732838. http://www.blackwell-synergy.com/openurl?genre=article&sid=nlm:pubmed&issn=0017-8748&date=2006&volume=46&issue=6&spage=925. Retrieved 2008-08-24.
- ^ Ceccarelli I, De Padova AM, Fiorenzani P, Massafra C, Aloisi AM (July 2006). "Single opioid administration modifies gonadal steroids in both the CNS and plasma of male rats". Neuroscience 140 (3): 929–37. doi:10.1016/j.neuroscience.2006.02.044. PMID 16580783. http://linkinghub.elsevier.com/retrieve/pii/S0306-4522(06)00277-6. Retrieved 2008-08-24.
- ^ May A, Bahra A, Büchel C, Frackowiak RS, Goadsby PJ (November 2000). "PET and MRA findings in cluster headache and MRA in experimental pain". Neurology 55 (9): 1328–35. PMID 11087776. http://www.neurology.org/cgi/pmidlookup?view=long&pmid=11087776.
- ^ DaSilva AF, Goadsby PJ, Borsook D (April 2007). "Cluster headache: a review of neuroimaging findings". Curr Pain Headache Rep 11 (2): 131–6. doi:10.1007/s11916-007-0010-1. PMID 17367592.
- ^ Pinessi L, Rainero I, Rivoiro C, Rubino E, Gallone S (September 2005 2005). "Genetics of cluster headache: an update". J Headache Pain 6 (4): 234–6. doi:10.1007/s10194-005-0194-x. PMID 16362673.
- ^ Schürks M, Diener HC (April 2008). "Cluster headache and lifestyle habits". Curr Pain Headache Rep 12 (2): 115–21. doi:10.1007/s11916-008-0022-5. PMID 18474191.
- ^ "Vast Majority of Cluster Headache Patients Are Initially Misdiagnosed, Dutch Researchers Report". World Headache Alliance. 2003-08-21. Archived from the original on 25 September 2006. http://web.archive.org/web/20060925093857/http://www.w-h-a.org/wha2/Newsite/resultsnav.asp?color=C2D9F2&idContentNews=595. Retrieved 2006-10-08.
- ^ NEURO/67 at eMedicine
- ^ "Seizures and Headaches: They Don't Have to Go Together". Epilepsy.com. 2003-09-16. http://www.epilepsy.com/articles/ar_1063754930.html. Retrieved 2006-09-22.
- ^ a b c May A, Leone M, Afra J, Linde M, Sándor P, Evers S, Goadsby P (October 2006). "EFNS guidelines on the treatment of cluster headache and other trigeminal-autonomic cephalalgias". Eur J Neurol 13 (10): 1066–77. doi:10.1111/j.1468-1331.2006.01566.x. PMID 16987158. Free Full Text (PDF)
- ^ Mauskop, Alexander; Altura, Bella T.; Cracco, Roger Q.; Altura, Burton M. (1995). "Intravenous magnesium sulfate relieves cluster headaches in patients with low serum ionized magnesium levels". Headache 35 (10): 597–600. doi:10.1111/j.1526-4610.1995.hed3510597.x. PMID 8550360.
- ^ Leone M, et al. (19965). "Melatonin versus placebo in the prophylaxis of cluster headache: a double-blind pilot study with parallel groups". Cephalalgia 16 (7): 494–496. doi:10.1046/j.1468-2982.1996.1607494.x. PMID 8933994.
- ^ Cohen AS, Burns B, Goadsby PJ (December 2009). "High-flow oxygen for treatment of cluster headache: a randomized trial". JAMA 302 (22): 2451–7. doi:10.1001/jama.2009.1855. PMID 19996400.
- ^ Cohen AS, Burns B, Goadsby PJ (December 2009). "High-flow oxygen for treatment of cluster headache: a randomized trial". JAMA 302 (22): 2451–7. doi:10.1001/jama.2009.1855. PMID 19996400.
- ^ Bennett MH, French C, Schnabel A, Wasiak J, Kranke P (2008). Normobaric and hyperbaric oxygen therapy for migraine and cluster headache. In Bennett, Michael H. "Cochrane Database of Systematic Reviews". Cochrane Database of Systematic Reviews (3): CD005219. doi:10.1002/14651858.CD005219.pub2. PMID 18646121.
- ^ Nilsson Remahl AI, Ansjön R, Lind F, Waldenlind E (November 2002). "Hyperbaric oxygen treatment of active cluster headache: a double-blind placebo-controlled cross-over study". Cephalalgia 22 (9): 730–9. doi:10.1046/j.1468-2982.2002.00450.x. PMID 12421159. http://www.blackwell-synergy.com/openurl?genre=article&sid=nlm:pubmed&issn=0333-1024&date=2002&volume=22&issue=9&spage=730. Retrieved 2008-08-22.
- ^ Di Sabato F, Rocco M, Martelletti P, Giacovazzo M (June 1997). "Hyperbaric oxygen in chronic cluster headaches: influence on serotonergic pathways". Undersea Hyperb Med 24 (2): 117–22. PMID 9171470. http://archive.rubicon-foundation.org/2253. Retrieved 2008-08-22.
- ^ Law S, Derry S, Moore RA (2010). Triptans for acute cluster headache. In Law, Simon. "Cochrane Database of Systematic Reviews". Cochrane Database Syst Rev 4 (4): CD008042. doi:10.1002/14651858.CD008042.pub2. PMID 20393964.
- ^ Sostak P, Krause P, Förderreuther S, Reinisch V, Straube A (September 2007). "Botulinum toxin type-A therapy in cluster headache: an open study". J Headache Pain 8 (4): 236–41. doi:10.1007/s10194-007-0400-0. PMID 17901920.
- ^ "Interview with Dr. Jeff Baird: Treating Migraines with Medical Acupuncture". American Academy of Medical Acupuncture.. http://www.medicalacupuncture.org/acu_info/interviews/baird.html. Retrieved 2008-08-24.
- ^ Mills T, Scoggin J (Jul-Aug 1997). "Intranasal lidocaine for migraine and cluster headaches". Ann Pharmacother 31 (7–8): 914–5. PMID 9220056.
- ^ The Treatment of Cluster Headaches Using 2-Bromo-Lysergic Acid Diethylamide. The Beckley Foundation
- ^ "Cluster headache may respond to kudzu products". Reuters. 2 February 2009. http://www.reuters.com/article/2009/02/02/us-cluster-headache-kudzu-idUSTRE51162Y20090202.
- ^ Ekbom K, Lindahl J (1970). "Effect of induced rise of blood pressure on pain in cluster headache". Acta Neurol Scand 46 (4): 585–600. doi:10.1111/j.1600-0404.1970.tb05815.x. PMID 4994083.
- ^ Atkinson R (November 1977). "Physical fitness and headache". Headache 17 (5): 189–91. doi:10.1111/j.1526-4610.1977.hed1705189.x. PMID 924787.
- ^ Gotkine M, Steiner I, Biran I. (November 2006). "Now dear, I have a headache! Immediate improvement of cluster headaches after sexual activity". J Neurol Neurosurg Psychiatry. 77 (11): 1296. doi:10.1136/jnnp.2006.092643. PMC 2077391. PMID 17043304. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2077391.- Abstract
- ^ http://www.diamondheadache.com/article_archives/cluster_headache.html
- ^ Torelli P, Castellini P, Cucurachi L, Devetak M, Lambru G, Manzoni G (2006). "Cluster headache prevalence: methodological considerations. A review of the literature". Acta Biomed Ateneo Parmense 77 (1): 4–9. PMID 16856701.
- ^ Harris W.: Neuritis and Neuralgia. Oxford: Oxford Univ.Press; 1926
- ^ Bickerstaff ER (May 1959). "The periodic migrainous neuralgia of Wilfred Harris". Lancet 1 (7082): 1069–71. doi:10.1016/S0140-6736(59)90651-8. PMID 13655672.
- ^ Boes CJ, Capobianco DJ, Matharu MS, Goadsby PJ (May 2002). "Wilfred Harris' early description of cluster headache". Cephalalgia 22 (4): 320–6. doi:10.1046/j.1468-2982.2002.00360.x. PMID 12100097.
- ^ Stephen D. Silberstein, Richard B. Lipton. Peter J. Goadsgy. "Headache in Clinical Practice." Second edition. Taylor & Francis. 2002.
- ^ Kittrelle JP, Grouse DS, Seybold ME (May 1985). "Cluster headache. Local anesthetic abortive agents". Arch. Neurol. 42 (5): 496–8. PMID 3994568.
- ^ Costa A, Pucci E, Antonaci F, et al. (March 2000). "The effect of intranasal cocaine and lidocaine on nitroglycerin-induced attacks in cluster headache". Cephalalgia 20 (2): 85–91. doi:10.1046/j.1468-2982.2000.00026.x. PMID 10961763.
External links
- ClusterHeadacheInfo.org - Cluster Headache Information, Discussion, Support
- Clusterheadaches.com.au - worldwide cluster headache information & support group
- http://www.clusterheadache.org
- Clusterheadaches.com, worldwide cluster headache support group
- Algorithm for diagnosis and treatment from National Guideline Clearinghouse (DHHS)
- The International Headache Society (IHS): 2nd Edition of The International Headache Classification (ICHD-2) - 3.1 Cluster Headache
- Organisation for the Understanding of Cluster Headache (UK)
- Association Française Contre l'Algie Vasculaire de la Face (FR)
- European ClusterHeads Alliance
- The City of London Migraine Clinic video on Cluster Headache
- The City of London Migraine Clinic video on Suicide Headache
- Video of a cluster headache attack
CNS disease: Headache (G43–G44, 339, 346) Primary ICHD 1ICHD 2ICHD 3ICHD 4Secondary ICHD 7ICHD 8ICHD 13 Other Categories:- Ailments of unknown etiology
- Headaches









Wikimedia Foundation. 2010.