- Rheumatic fever
-
Rheumatic fever Classification and external resources 
Streptococcus pyogenes bacteria, Pappenheim's stainICD-10 I00-I02 ICD-9 390–392 DiseasesDB 11487 MedlinePlus 003940 eMedicine med/3435 med/2922 emerg/509 ped/2006 MeSH D012213 Rheumatic fever is an inflammatory disease that occurs following a Streptococcus pyogenes infection, such as strep throat or scarlet fever. Believed to be caused by antibody cross-reactivity that can involve the heart, joints, skin, and brain,[1] the illness typically develops two to three weeks after a streptococcal infection. Acute rheumatic fever commonly appears in children between the ages of 6 and 15, with only 20% of first-time attacks occurring in adults.[1] The illness is so named because of its similarity in presentation to rheumatism.[2]
Contents
Diagnosis
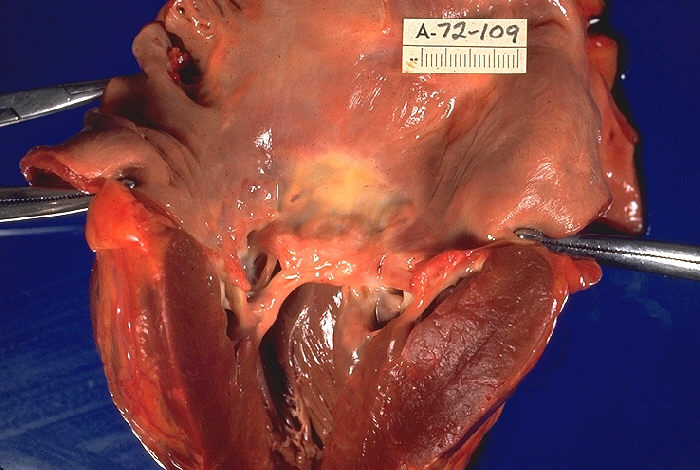
 Rheumatic heart disease at autopsy with characteristic findings (thickened mitral valve, thickened chordae tendineae, hypertrophied left ventricular myocardium).
Rheumatic heart disease at autopsy with characteristic findings (thickened mitral valve, thickened chordae tendineae, hypertrophied left ventricular myocardium).
Modified Jones criteria were first published in 1944 by T. Duckett Jones, MD.[3] They have been periodically revised by the American Heart Association in collaboration with other groups.[4] According to revised Jones criteria, the diagnosis of rheumatic fever can be made when two of the major criteria, or one major criterion plus two minor criteria, are present along with evidence of streptococcal infection: elevated or rising antistreptolysin O titre or DNAase.[1] Exceptions are chorea and indolent carditis, each of which by itself can indicate rheumatic fever.[5][6][7]
Major criteria
- polyarthritis: a temporary migrating inflammation of the large joints, usually starting in the legs and migrating upwards.
- Carditis: inflammation of the heart muscle which can manifest as congestive heart failure with shortness of breath, pericarditis with a rub, or a new heart murmur.
- Subcutaneous nodules: painless, firm collections of collagen fibers over bones or tendons. They commonly appear on the back of the wrist, the outside elbow, and the front of the knees.
- Erythema marginatum: a long lasting rash that begins on the trunk or arms as macules and spreads outward to form a snake like ring while clearing in the middle. This rash never starts on the face and it is made worse with heat.
- Sydenham's chorea (St. Vitus' dance): a characteristic series of rapid movements without purpose of the face and arms. This can occur very late in the disease for at least three months from onset of infection.
Minor criteria
- Fever of 38.2–38.9 °C (101–102 °F)
- Arthralgia: Joint pain without swelling (Cannot be included if polyarthritis is present as a major symptom)
- Raised erythrocyte sedimentation rate or C reactive protein
- Leukocytosis
- ECG showing features of heart block, such as a prolonged PR interval[8] (Cannot be included if carditis is present as a major symptom)
- First Degree AV-Block [9]
- Previous episode of rheumatic fever or inactive heart disease
Other signs and symptoms
- Abdominal pain
- Nose bleeds
- Preceding streptococcal infection: recent scarlet fever, raised antistreptolysin 0 or other streptococcal antibody titre, or positive throat culture.[9]
Pathophysiology
 Pathophysiology of rheumatic heart disease
Pathophysiology of rheumatic heart diseaseRheumatic fever is a systemic disease affecting the peri-arteriolar connective tissue and can occur after an untreated Group A Beta hemolytic streptococcal pharyngeal infection. It is believed to be caused by antibody cross-reactivity. This cross-reactivity is a Type II hypersensitivity reaction and is termed molecular mimicry. Usually, self reactive B cells remain anergic in the periphery without T cell co-stimulation. During a Streptococcus infection, mature antigen presenting cells such as B cells present the bacterial antigen to CD4-T cells which differentiate into helper T2 cells. Helper T2 cells subsequently activate the B cells to become plasma cells and induce the production of antibodies against the cell wall of Streptococcus. However the antibodies may also react against the myocardium and joints,[10] producing the symptoms of rheumatic fever.
Group A streptococcus pyogenes has a cell wall composed of branched polymers which sometimes contain M protein that are highly antigenic. The antibodies which the immune system generates against the M protein may cross react with cardiac myofiber protein myosin,[11] heart muscle glycogen and smooth muscle cells of arteries, inducing cytokine release and tissue destruction. However, the only proven cross reaction is with perivascular connective tissue.[citation needed] This inflammation occurs through direct attachment of complement and Fc receptor-mediated recruitment of neutrophils and macrophages. Characteristic Aschoff bodies, composed of swollen eosinophilic collagen surrounded by lymphocytes and macrophages can be seen on light microscopy. The larger macrophages may become Aschoff giant cells. Acute rheumatic valvular lesions may also involve a cell-mediated immunity reaction as these lesions predominantly contain T-helper cells and macrophages.[12]
In acute rheumatic fever, these lesions can be found in any layer of the heart and is hence called pancarditis. The inflammation may cause a serofibrinous pericardial exudate described as "bread-and-butter" pericarditis, which usually resolves without sequelae. Involvement of the endocardium typically results in fibrinoid necrosis and verrucae formation along the lines of closure of the left-sided heart valves. Warty projections arise from the deposition, while subendothelial lesions may induce irregular thickenings called MacCallum plaques.
Chronic rheumatic heart disease is characterized by repeated inflammation with fibrinous resolution. The cardinal anatomic changes of the valve include leaflet thickening, commissural fusion and shortening and thickening of the tendinous cords.[12]
Prevention
Prevention of recurrence is achieved by eradicating the acute infection and prophylaxis with antibiotics. The American Heart Association recommends daily or monthly prophylaxis continue long-term, perhaps for life.[13][dead link]
Treatment
The management of acute rheumatic fever is geared toward the reduction of inflammation with anti-inflammatory medications such as aspirin or corticosteroids. Individuals with positive cultures for strep throat should also be treated with antibiotics. Aspirin is the drug of choice and should be given at high doses of 100 mg/kg/day. One should watch for side effects like gastritis and salicylate poisoning. In children and teenagers, the use of aspirin and aspirin-containing products can be associated with Reye's syndrome, a serious and potentially deadly condition. The risks, benefits and alternative treatments must always be considered when administering aspirin and aspirin-containing products in children and teenagers. Ibuprofen for pain and discomfort and corticosteroids for moderate to severe inflammatory reactions manifested by rheumatic fever should be considered in children and teenagers. Steroids are reserved for cases where there is evidence of involvement of heart. The use of steroids may prevent further scarring of tissue and may prevent development of sequelae such as mitral stenosis. Monthly injections of longacting penicillin must be given for a period of five years in patients having one attack of rheumatic fever. If there is evidence of carditis, the length of Penidure therapy may be up to 40 years. Another important cornerstone in treating rheumatic fever includes the continual use of low-dose antibiotics (such as penicillin, sulfadiazine, or erythromycin) to prevent recurrence.
Infection
Patients with positive cultures for Streptococcus pyogenes should be treated with penicillin as long as allergy is not present. This treatment will not alter the course of the acute disease.
The most appropriate treatment stated in the Oxford Handbook of Clinical Medicine for rheumatic fever is benzathine benzylpenicillin.
Inflammation
Patients with significant symptoms may require corticosteroids. Salicylates are useful for pain.
Heart failure
Some patients develop significant carditis which manifests as congestive heart failure. This requires the usual treatment for heart failure: diuretics and digoxin. Unlike normal heart failure, rheumatic heart failure responds well to corticosteroids.
Epidemiology
 Disability-adjusted life year for rheumatic heart disease per 100,000 inhabitants in 2004.[14]no dataless than 2020-4040-6060-8080-100100-120120-140140-160160-180180-200200-330more than 330
Disability-adjusted life year for rheumatic heart disease per 100,000 inhabitants in 2004.[14]no dataless than 2020-4040-6060-8080-100100-120120-140140-160160-180180-200200-330more than 330Rheumatic fever is common worldwide and responsible for many cases of damaged heart valves. In Western countries, it became fairly rare since the 1960s, probably due to widespread use of antibiotics to treat streptococcus infections. While it has been far less common in the United States since the beginning of the 20th century, there have been a few outbreaks since the 1980s. Although the disease seldom occurs, it is serious and has a case-fatality rate of 2–5%.[15]
Rheumatic fever primarily affects children between ages 5 and 17 years and occurs approximately 20 days after strep throat. In up to a third of cases, the underlying strep infection may not have caused any symptoms.
The rate of development of rheumatic fever in individuals with untreated strep infection is estimated to be 3%. The incidence of recurrence with a subsequent untreated infection is substantially greater (about 50%).[16] The rate of development is far lower in individuals who have received antibiotic treatment. Persons who have suffered a case of rheumatic fever have a tendency to develop flare-ups with repeated strep infections.
The recurrence of rheumatic fever is relatively common in the absence of maintenance of low dose antibiotics, especially during the first three to five years after the first episode. Heart complications may be long-term and severe, particularly if valves are involved.
Survivors of rheumatic fever often have to take penicillin to prevent streptococcal infection which could possibly lead to another case of rheumatic fever that could prove fatal.
References
- ^ a b c Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; & Mitchell, Richard N. (2007). Robbins Basic Pathology (8th ed.). Saunders Elsevier. pp. 403-406 ISBN 978-1-4160-2973-1
- ^ "rheumatic fever" at Dorland's Medical Dictionary
- ^ Jones TD (1944). "The diagnosis of rheumatic fever.". JAMA 126: 481–4.
- ^ Ferrieri P; Jones Criteria Working, Group (2002). "Proceedings of the Jones Criteria workshop". Circulation 106 (19): 2521–3. doi:10.1161/01.CIR.0000037745.65929.FA. PMID 12417554. http://circ.ahajournals.org/cgi/content/full/106/19/2521?ck=nck.
- ^ Steven J Parrillo, DO, FACOEP, FACEP. "eMedicine — Rheumatic Fever". http://www.emedicine.com/emerg/topic509.htm. Retrieved 2007-07-14.
- ^ "Guidelines for the diagnosis of rheumatic fever. Jones Criteria, 1992 update. Special Writing Group of the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young of the American Heart Association". JAMA 268 (15): 2069–73. 1992. doi:10.1001/jama.268.15.2069. PMID 1404745.
- ^ Saxena, Anita (2000). "Diagnosis of rheumatic fever: Current status of Jones criteria and role of echocardiography". Indian Journal of Pediatrics 67 (4): 283–6. doi:10.1007/BF02758174. PMID 11129913.
- ^ Aly, Ashraf (2008). "Rheumatic Fever". Core Concepts of Pediatrics. University of Texas. http://www.utmb.edu/pedi_ed/CORE/Cardiology/page_40.htm. Retrieved 2011-08-06.
- ^ a b Ed Boon, Davidson's General Practice of Medicine, 20th edition. P. 617.
- ^ Abbas, Abul K.; Lichtman, Andrew H.; Baker, David L.; et al (2004). Basic immunology: functions and disorders of the immune system (2 ed.). Philadelphia, Pennsylvania: Elsevier Saunders. ISBN 978-1416024033.
- ^ Faé KC, da Silva DD, Oshiro SE, et al. (May 2006). "Mimicry in recognition of cardiac myosin peptides by heart-intralesional T cell clones from rheumatic heart disease". J. Immunol. 176 (9): 5662–70. PMID 16622036. http://www.jimmunol.org/cgi/pmidlookup?view=long&pmid=16622036.
- ^ a b Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease. St. Louis, Mo: Elsevier Saunders. ISBN 0-7216-0187-1. http://www.robbinspathology.com/.
- ^ "Rheumatic Heart Disease/Rheumatic Fever". American Heart Association. http://www.americanheart.org/presenter.jhtml?identifier=4709. Retrieved 2008-02-17.
- ^ "WHO Disease and injury country estimates". World Health Organization. 2009. http://www.who.int/healthinfo/global_burden_disease/estimates_country/en/index.html. Retrieved Nov. 11, 2009.
- ^ NLM/NIH: Medline Plus Medical Encyclopedia: Rheumatic fever
- ^ Porth, Carol (2007). Essentials of pathophysiology: concepts of altered health states. Hagerstown, MD: Lippincott Williams & Wilkins. ISBN 0-7817-7087-4.
External links
- Rheumatic fever information from Seattle Children's Hospital Heart Center
- Jones major criteria, Mnemonic
- Rheumatic Heart Disease Network
Firmicutes (low-G+C) Infectious diseases · Bacterial diseases: G+ (primarily A00–A79, 001–041, 080–109) Bacilli Streptococcusαoptochin susceptible: S. pneumoniae (Pneumococcal infection)optochin resistant: S. viridans: S. mitis, S. mutans, S. oralis, S. sanguinis, S. sobrinus, milleri groupβA, bacitracin susceptible: S. pyogenes (Scarlet fever, Erysipelas, Rheumatic fever, Streptococcal pharyngitis)B, bacitracin resistant, CAMP test+: S. agalactiaeungrouped: Streptococcus iniae (Cutaneous Streptococcus iniae infection)Clostridia Clostridium (spore-forming)Peptostreptococcus (non-spore forming)Peptostreptococcus magnusMollicutes MycoplasmataceaeUreaplasma urealyticum (Ureaplasma infection) · Mycoplasma genitalium · Mycoplasma pneumoniae (Mycoplasma pneumonia)Erysipelothrix rhusiopathiae (Erysipeloid)Immune disorders: hypersensitivity and autoimmune diseases (279.5–6) Type I/allergy/atopy
(IgE)ForeignAtopic dermatitis · Allergic urticaria · Hay fever · Allergic asthma · Anaphylaxis · Food allergy (Milk, Egg, Peanut, Tree nut, Seafood, Soy, Wheat), Penicillin allergyAutoimmunenoneType II/ADCC
(IgM, IgG)ForeignAutoimmuneAutoimmune hemolytic anemia · Idiopathic thrombocytopenic purpura · Bullous pemphigoid · Pemphigus vulgaris · Rheumatic fever · Goodpasture's syndromeType III
(Immune complex)ForeignHenoch–Schönlein purpura · Hypersensitivity vasculitis · Reactive arthritis · Rheumatoid arthritis · Farmer's lung · Post-streptococcal glomerulonephritis · Serum sickness · Arthus reactionAutoimmuneType IV/cell-mediated
(T-cells)ForeignAllergic contact dermatitis · Mantoux testAutoimmuneUnknown/
multipleForeignAutoimmuneSjögren's syndrome · Autoimmune hepatitis · Autoimmune polyendocrine syndrome (APS1, APS2) · Autoimmune adrenalitis · Systemic autoimmune diseaseCategories:- Rheumatology
- Chronic rheumatic heart diseases
- Inflammations



Wikimedia Foundation. 2010.