- Crohn's disease
-
Crohn's disease Classification and external resources
ileal, ileocolic and colonic.[1]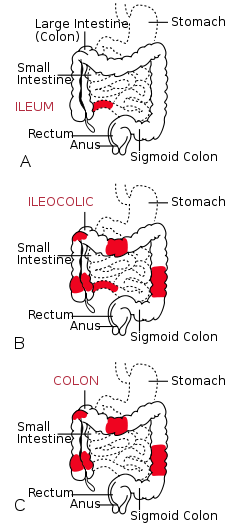
The three most common sites of intestinal involvement in Crohn's disease areICD-10 K50 ICD-9 555 OMIM 266600 DiseasesDB 3178 MedlinePlus 000249 eMedicine med/477 ped/507 radio/197 MeSH D003424 Crohn's disease, also known as regional enteritis, is a type of inflammatory bowel disease that may affect any part of the gastrointestinal tract from mouth to anus, causing a wide variety of symptoms. It primarily causes abdominal pain, diarrhea (which may be bloody if inflammation is at its worst), vomiting (can be continuous), or weight loss,[1][2][3] but may also cause complications outside the gastrointestinal tract such as skin rashes, arthritis, inflammation of the eye, tiredness, and lack of concentration.[1]
Poorly understood interactions between environmental, immunological and bacterial factors play a role in causing Crohn's disease.[4][5][6] This results in a chronic inflammatory disorder, in which the body's immune system attacks the gastrointestinal tract possibly directed at a microbial antigens.[7][5] There is evidence of a genetic link to Crohn's disease, putting individuals with siblings afflicted with the disease at higher risk.[8] Males and females are equally affected. Smokers are two times more likely to develop Crohn's disease than nonsmokers.[9] Crohn's disease affects between 400,000 and 600,000 people in North America.[10] Prevalence estimates for Northern Europe have ranged from 27–48 per 100,000.[11] Crohn's disease tends to present initially in the teens and twenties, with another peak incidence in the fifties to seventies, although the disease can occur at any age.[1][12] There is no known pharmaceutical or surgical cure for Crohn's disease.[13] Treatment options are restricted to controlling symptoms, maintaining remission, and preventing relapse.
The disease was named after American gastroenterologist Burrill Bernard Crohn, who, in 1932, together with two colleagues, described a series of patients with inflammation of the terminal ileum, the area most commonly affected by the illness.[14] For this reason, the disease has also been called regional ileitis[14] or regional enteritis. The condition, however, had previously been independently described in medical literature by others. The most notable case was in 1904 by Polish surgeon Antoni Leśniowski for whom the condition is alternatively named Leśniowski-Crohn's disease in Polish literature.
Contents
Classification
 Distribution of gastrointestinal Crohn's disease. Based on data from American Gastroenterological Association.
Distribution of gastrointestinal Crohn's disease. Based on data from American Gastroenterological Association.
Crohn's disease is one type of inflammatory bowel disease (IBD). It typically manifests in the gastrointestinal tract and can be categorized by the specific tract region affected. A disease of both the ileum (the last part of the small intestine, which connects to the large intestine), and the large intestine, Ileocolic Crohn's accounts for fifty percent of cases. Crohn's ileitis, manifest in the ileum only, accounts for thirty percent of cases, while Crohn's colitis, of the large intestine, accounts for the remaining twenty percent of cases and may be particularly difficult to distinguish from ulcerative colitis. Gastroduodenal Crohn's disease causes inflammation in the stomach and first part of the small intestine, called the duodenum. Jejunoileitis causes spotty patches of inflammation in the top half of the small intestine, called the jejunum (MedlinePlus 2010). The disease can attack any part of the digestive tract, from mouth to anus. However, individuals affected by the disease rarely fall outside these three classifications, with presentations in other areas.[1]
Crohn's disease may also be categorized by the behavior of disease as it progresses. These categorizations formalized in the Vienna classification of the disease.[15] There are three categories of disease presentation in Crohn's disease: stricturing, penetrating, and inflammatory. Stricturing disease causes narrowing of the bowel that may lead to bowel obstruction or changes in the caliber of the feces. Penetrating disease creates abnormal passageways (fistulae) between the bowel and other structures, such as the skin. Inflammatory disease (or nonstricturing, nonpenetrating disease) causes inflammation without causing strictures or fistulae.[15][16]
Signs and symptoms
Symptoms in Crohn's disease vs. ulcerative colitis () Crohn's disease Ulcerative colitis Defecation Often porridge-like[17],
sometimes steatorrheaOften mucus-like
and with blood[17]Tenesmus Less common[17] More common[17] Fever Common[17] Indicates severe disease[17] Fistulae Common[18] Seldom Weight loss Often More seldom Gastrointestinal

Many people with Crohn's disease have symptoms for years prior to the diagnosis.[19] The usual onset is between 15 and 30 years of age, but can occur at any age.[20] Because of the 'patchy' nature of the gastrointestinal disease and the depth of tissue involvement, initial symptoms can be more subtle than those of ulcerative colitis. People with Crohn's disease experience chronic recurring periods of flare-ups and remission.[21]
Abdominal pain may be the initial symptom of Crohn's disease. It is often accompanied by diarrhea, especially in those who have had surgery. The diarrhea may or may not be bloody. People who have had surgery or multiple surgeries often end up with short bowel syndrome of the gastrointestinal tract. The nature of the diarrhea in Crohn's disease depends on the part of the small intestine or colon involved. Ileitis typically results in large-volume, watery feces. Colitis may result in a smaller volume of feces of higher frequency. Fecal consistency may range from solid to watery. In severe cases, an individual may have more than 20 bowel movements per day and may need to awaken at night to defecate.[1][12][22][23] Visible bleeding in the feces is less common in Crohn's disease than in ulcerative colitis, but may be seen in the setting of Crohn's colitis.[1] Bloody bowel movements are typically intermittent, and may be bright or dark red in color. In the setting of severe Crohn's colitis, bleeding may be copious.[12] Flatulence and bloating may also add to the intestinal discomfort.[12]
Symptoms caused by intestinal stenosis are also common in Crohn's disease. Abdominal pain is often most severe in areas of the bowel with stenoses. In the setting of severe stenosis, vomiting and nausea may indicate the beginnings of small bowel obstruction.[12] Although the association is greater in the context of ulcerative colitis, Crohn's disease may also be associated with primary sclerosing cholangitis, a type of inflammation of the bile ducts.[24]
Perianal discomfort may also be prominent in Crohn's disease. Itchiness or pain around the anus may be suggestive of inflammation, fistulization or abscess around the anal area[1] or anal fissure. Perianal skin tags are also common in Crohn's disease.[25] Fecal incontinence may accompany perianal Crohn's disease. At the opposite end of the gastrointestinal tract, the mouth may be affected by non-healing sores (aphthous ulcers). Rarely, the esophagus, and stomach may be involved in Crohn's disease. These can cause symptoms including difficulty swallowing (dysphagia), upper abdominal pain, and vomiting.[26]
Systemic
Crohn's disease, like many other chronic, inflammatory diseases, can cause a variety of systemic symptoms.[1] Among children, growth failure is common. Many children are first diagnosed with Crohn's disease based on inability to maintain growth.[27] As it may manifest at the time of the growth spurt in puberty, up to 30% of children with Crohn's disease may have retardation of growth.[28] Fever may also be present, though fevers greater than 38.5 ˚C (101.3 ˚F) are uncommon unless there is a complication such as an abscess.[1] Among older individuals, Crohn's disease may manifest as weight loss, usually related to decreased food intake, since individuals with intestinal symptoms from Crohn's disease often feel better when they do not eat and might lose their appetite.[27] People with extensive small intestine disease may also have malabsorption of carbohydrates or lipids, which can further exacerbate weight loss.[29]
Extraintestinal
 Erythema nodosum on the back of a person with Crohn's disease
Erythema nodosum on the back of a person with Crohn's diseaseIn addition to systemic and gastrointestinal involvement, Crohn's disease can affect many other organ systems.[30] Inflammation of the interior portion of the eye, known as uveitis, can cause eye pain, especially when exposed to light (photophobia). Inflammation may also involve the white part of the eye (sclera), a condition called episcleritis. Both episcleritis and uveitis can lead to loss of vision if untreated.
Crohn's disease is associated with a type of rheumatologic disease known as seronegative spondyloarthropathy. This group of diseases is characterized by inflammation of one or more joints (arthritis) or muscle insertions (enthesitis). The arthritis can affect larger joints, such as the knee or shoulder, or may exclusively involve the small joints of the hands and feet. The arthritis may also involve the spine, leading to ankylosing spondylitis if the entire spine is involved or simply sacroiliitis if only the lower spine is involved. The symptoms of arthritis include painful, warm, swollen, stiff joints and loss of joint mobility or function.[21]
 Pyoderma gangrenosum on the leg of a person with Crohn's disease
Pyoderma gangrenosum on the leg of a person with Crohn's diseaseCrohn's disease may also involve the skin, blood, and endocrine system. One type of skin manifestation, erythema nodosum, presents as red nodules usually appearing on the shins. Erythema nodosum is due to inflammation of the underlying subcutaneous tissue, and is characterized by septal panniculitis. Another skin lesion, pyoderma gangrenosum, is typically a painful ulcerating nodule. Crohn's disease also increases the risk of blood clots; painful swelling of the lower legs can be a sign of deep venous thrombosis, while difficulty breathing may be a result of pulmonary embolism. Autoimmune hemolytic anemia, a condition in which the immune system attacks the red blood cells, is also more common in Crohn's disease and may cause fatigue, pallor, and other symptoms common in anemia. Clubbing, a deformity of the ends of the fingers, may also be a result of Crohn's disease. Finally, Crohn's disease may cause osteoporosis, or thinning of the bones. Individuals with osteoporosis are at increased risk of bone fractures.[11]
Crohn's disease can also cause neurological complications (reportedly in up to 15% of patients).[31] The most common of these are seizures, stroke, myopathy, peripheral neuropathy, headache and depression.[31]
Crohn's patients often also have issues with small bowel bacterial overgrowth syndrome, which has similar symptoms.[32]
In the oral cavity crohn's patients may suffer from cheilitis granulomatosa and other forms of orofacial granulomatosis, pyostomatitis vegetans, recurrent aphthous stomatitis, geographic tongue and migratory stomatitis in higher prevalence than the general population.[33]
Complications
Complications of Crohn's disease vs. ulcerative colitis
Crohn's disease Ulcerative colitis Nutrient deficiency Higher risk Colon cancer risk Slight Considerable Prevalence of
extraintestinal complications[34]Iritis/uveitis Females 2.2% 3.2% Males 1.3% 0.9% Primary sclerosing
cholangitisFemales 0.3% 1% Males 0.4% 3% Ankylosing
spondylitisFemales 0.7% 0.8% Males 2.7% 1.5% Pyoderma
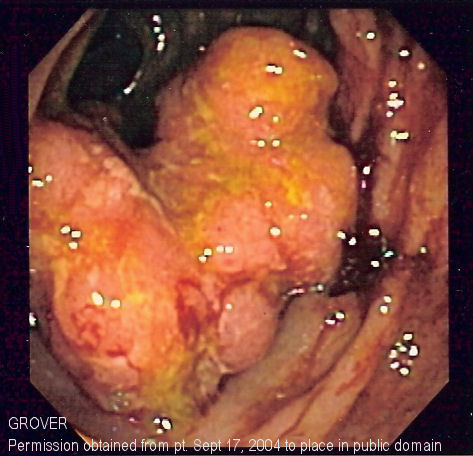
gangrenosumFemales 1.2% 0.8% Males 1.3% 0.7% Erythema nodosum Females 1.9% 2% Males 0.6% 0.7%  Endoscopic image of colon cancer identified in the sigmoid colon on screening colonoscopy for Crohn's disease
Endoscopic image of colon cancer identified in the sigmoid colon on screening colonoscopy for Crohn's diseaseCrohn's disease can lead to several mechanical complications within the intestines, including obstruction, fistulae, and abscesses. Obstruction typically occurs from strictures or adhesions that narrow the lumen, blocking the passage of the intestinal contents. Fistulae can develop between two loops of bowel, between the bowel and bladder, between the bowel and vagina, and between the bowel and skin. Abscesses are walled off collections of infection, which can occur in the abdomen or in the perianal area in Crohn's disease sufferers. Crohn's is responsible for 10% of vesicoenteric fistulae, and is the most common cause of ileovesical fistulae.[35]
Crohn's disease also increases the risk of cancer in the area of inflammation. For example, individuals with Crohn's disease involving the small bowel are at higher risk for small intestinal cancer. Similarly, people with Crohn's colitis have a relative risk of 5.6 for developing colon cancer.[36] Screening for colon cancer with colonoscopy is recommended for anyone who has had Crohn's colitis for at least eight years.[37] Some studies suggest there is a role for chemoprotection in the prevention of colorectal cancer in Crohn's involving the colon; two agents have been suggested, folate and mesalamine preparations.[38]
Individuals with Crohn's disease are at risk of malnutrition for many reasons, including decreased food intake and malabsorption. The risk increases following resection of the small bowel. Such individuals may require oral supplements to increase their caloric intake, or in severe cases, total parenteral nutrition (TPN). Most people with moderate or severe Crohn's disease are referred to a dietitian for assistance in nutrition.[39]
Crohn's disease can cause significant complications, including bowel obstruction, abscesses, free perforation and hemorrhage.[40]
Crohn's disease can be problematic during pregnancy, and some medications can cause adverse outcomes for the fetus or mother. Consultation with an obstetrician and gastroenterologist about Crohn's disease and all medications allows preventative measures to be taken. In some cases, remission can occur during pregnancy. Certain medications can also impact sperm count or may otherwise adversely affect a man's ability to conceive.[41]
Cause
Risk factors in Crohn's disease vs. ulcerative colitis.
Crohn's disease Ulcerative colitis Smoking Higher risk for smokers Lower risk for smokers[42] Age Usual onset between
15 and 30 years[43]Peak incidence between
15 and 25 yearsAlthough the exact cause of Crohn's disease is still unknown, a combination of environmental factors and genetic predisposition seems to cause the disease.[44] The genetic risk factors have now more or less been comprehensively elucidated, making Crohn's disease the first genetically complex disease of which the genetic background has been resolved.[45] The relative risks of contracting the disease when one has a mutation in one of the risk genes, however, are actually very low (approximately 1:200). In broad terms, the genetic data indicate the innate immune systems in patients with Crohn's disease malfunction, and direct assessment of patient immunity confirms this notion.[46] This had led to the notion Crohn's disease should be viewed as innate immune deficiency, chronic inflammation being caused by adaptive immunity trying to compensate for the reduced function of the innate immune system.[47]
Genetics
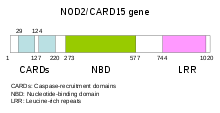 Schematic of NOD2 CARD15 gene, which is associated with certain disease patterns in Crohn's disease.
Schematic of NOD2 CARD15 gene, which is associated with certain disease patterns in Crohn's disease.Some research has indicated Crohn's disease may have a genetic link.[48] The disease runs in families and those with a sibling with the disease are 30 times more likely to develop it than the general population.
Mutations in the CARD15 gene (also known as the NOD2 gene) are associated with Crohn's disease[49] and with susceptibility to certain phenotypes of disease location and activity.[50] In earlier studies, only two genes were linked to Crohn's, but scientists now believe over thirty genes play a role in the disease, either directly through causation or indirectly, as with a mediator variable. Anomalies in the XBP1 gene have recently been identified as a factor, pointing towards a role for the unfolded protein response pathway of the endoplasmatic reticulum in inflammatory bowel diseases.[51][52]
Environmental factors
Diet is believed to be linked to its higher prevalence in industrialized parts of the world. A positive correlation has been found between the incidence of the disease and an increased intake of animal protein, milk protein and an increased ratio of omega-6 to omega-3 polyunsaturated fatty acids.[53] Negative correlation of the disease incidence was found in the increased consumption of vegetable protein, and no correlation to fish protein.[53] Smoking has been shown to increase the risk of the return of active disease, or "flares".[9] The introduction of hormonal contraception in the United States in the 1960s is linked with a dramatic increase in the incidence rate of Crohn's disease. Although a causal linkage has not been effectively shown, there remain fears these drugs work on the digestive system in ways similar to smoking.[54] Several scientific studies have posited isotretinoin is a possible cause of Crohn's disease in some individuals.[55][56][57] Emotional stress is also likely contribute to the progression and worsening of Crohn's disease.[58]
Immune system
Abnormalities in the immune system have often been invoked as being causes of Crohn's disease. It is thought to be an autoimmune disease, with inflammation stimulated by an overactive Th1 cytokine response.[59] However, more recent evidence has shown Th17 is of greater importance in the disease.[60] The most recent gene to be implicated in Crohn's disease is ATG16L1, which may induce autophagy and hinder the body's ability to attack invasive bacteria.[61]
Contrary to the prevailing view that Crohn's disease is a primary T cell autoimmune disorder, there is an increasing body of evidence in favor of the hypothesis that Crohn's disease results from an impaired innate immunity.[62] The immunodeficiency, which has been shown to be due (at least in part) to impaired cytokine secretion by macrophages, is thought to lead to a sustained microbial-induced inflammatory response, in particular, in the colon where the bacterial load is especially high.[46][63]
Microbes
A variety of pathogenic bacteria were initially suspected of being causative agents of Crohn's disease.[64] However, most healthcare professionals now believe a variety of microorganisms are taking advantage of their host's weakened mucosal layer and inability to clear bacteria from the intestinal walls, both symptoms of the disease.[65] Some studies have suggested Mycobacterium avium subspecies paratuberculosis (MAP) plays a role in Crohn's disease, in part because it causes a very similar disease, Johne's disease, in cattle.[66] The mannose-bearing antigens (mannins) from yeast may also elicit an antibody response.[67] Other studies have linked specific strains of enteroadherent E. coli to the disease.[68] Still, this relationship between specific types of bacteria and Crohn's disease remains unclear.[69][70]
Some studies have suggested some symptoms of Crohn's disease, ulcerative colitis and irritable bowel syndrome have the same underlying cause. Biopsy samples taken from the colons of all three patient groups were found to produce elevated levels of a serine protease.[71] Experimental introduction of the serine protease into mice has been found to produce widespread pain associated with irritable bowel syndrome, as well as colitis, which is associated with all three diseases.[72] The authors of that study were unable to identify the source of the protease, but a separate review noted regional and temporal variations in those illnesses follow those associated with infection with a poorly understood protozoan, Blastocystis.[73]
A study in 2003 put forth the "cold-chain" hypothesis that psychrotrophic bacteria such as Yersinia and Listeria species contribute to the disease. A statistical correlation was found between the advent of the use of refrigeration in the United States and various parts of Europe and the rise of the disease.[74][75] Later studies have provided support for this hypothesis.[76]
Studies done at the University of Liverpool have offered ideas to explain the apparent connection between Crohn's disease, Mycobacterium, other pathogenic bacteria, and genetic markers.[77][78] In many individuals, genetic factors predispose individuals to Mycobacterium avium subsp. paratuberculosis infection. This bacterium then produces mannins, which protect both itself and various bacteria from phagocytosis, which causes a variety of secondary infections.[79]
Pathophysiology
Pathophysiology in Crohn's disease vs. ulcerative colitis
Crohn's disease Ulcerative colitis Autoimmune disease Widely regarded as
an autoimmune diseaseNo consensus Cytokine response Associated with Th17[60] Vaguely associated with Th2  Section of colectomy showing transmural inflammation
Section of colectomy showing transmural inflammationDuring a colonoscopy, biopsies of the colon are often taken to confirm the diagnosis. Certain characteristic features of the pathology seen point toward Crohn's disease; it shows a transmural pattern of inflammation, meaning the inflammation may span the entire depth of the intestinal wall.[1] Ulceration is an outcome seen in highly active disease. There is usually an abrupt transition between unaffected tissue and the ulcer. Under a microscope, biopsies of the affected colon may show mucosal inflammation, characterized by focal infiltration of neutrophils, a type of inflammatory cell, into the epithelium. This typically occurs in the area overlying lymphoid aggregates. These neutrophils, along with mononuclear cells, may infiltrate the crypts, leading to inflammation (crypititis) or abscess (crypt abscess). Granulomas, aggregates of macrophage derivatives known as giant cells, are found in 50% of cases and are most specific for Crohn's disease. The granulomas of Crohn's disease do not show "caseation", a cheese-like appearance on microscopic examination characteristic of granulomas associated with infections, such as tuberculosis. Biopsies may also show chronic mucosal damage, as evidenced by blunting of the intestinal villi, atypical branching of the crypts, and a change in the tissue type (metaplasia). One example of such metaplasia, Paneth cell metaplasia, involves development of Paneth cells (typically found in the small intestine) in other parts of the gastrointestinal system.[80]
Diagnosis
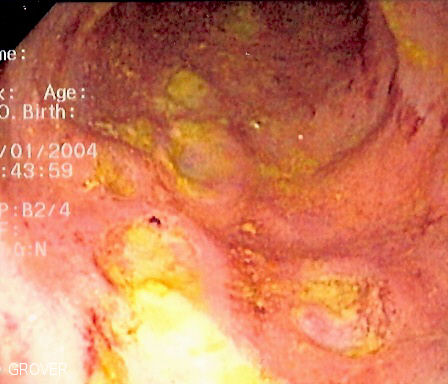
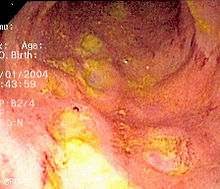 Endoscopic image of Crohn's colitis showing deep ulceration
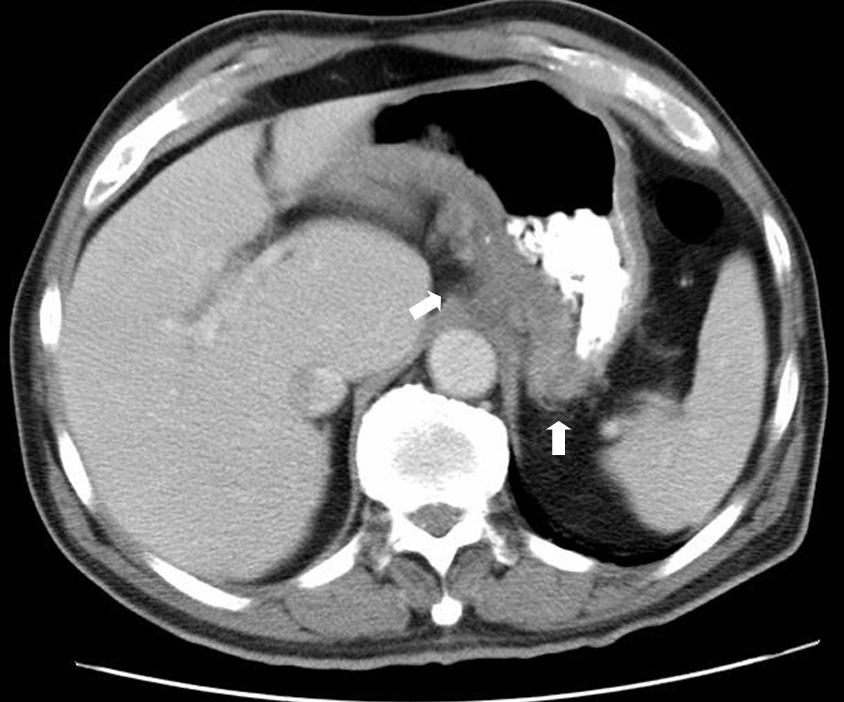
Endoscopic image of Crohn's colitis showing deep ulceration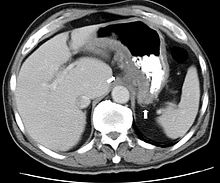 CT scan showing Crohn's disease in the fundus of the stomach
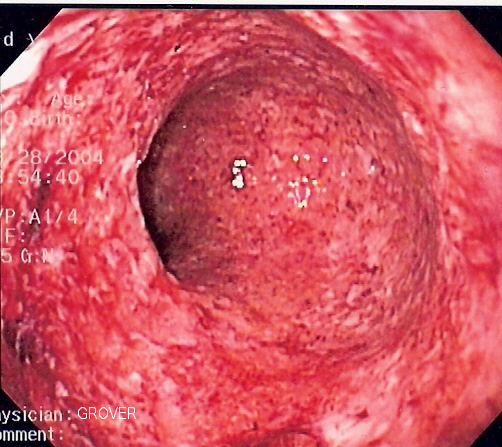
CT scan showing Crohn's disease in the fundus of the stomach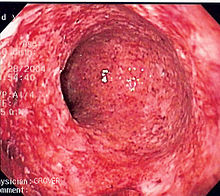 Crohn's disease can mimic ulcerative colitis on endoscopy. This endoscopic image is of Crohn's colitis showing diffuse loss of mucosal architecture, friability of mucosa in sigmoid colon and exudate on wall, all of which can be found with ulcerative colitis.
Crohn's disease can mimic ulcerative colitis on endoscopy. This endoscopic image is of Crohn's colitis showing diffuse loss of mucosal architecture, friability of mucosa in sigmoid colon and exudate on wall, all of which can be found with ulcerative colitis.The diagnosis of Crohn's disease can sometimes be challenging,[19] and a number of tests are often required to assist the physician in making the diagnosis.[12] Even with a full battery of tests, it may not be possible to diagnose Crohn's with complete certainty; a colonoscopy is approximately 70% effective in diagnosing the disease, with further tests being less effective. Disease in the small bowel is particularly difficult to diagnose, as a traditional colonoscopy allows access to only the colon and lower portions of the small intestines; introduction of the capsule endoscopy[81] aids in endoscopic diagnosis. Multinucleated giant cells, a common finding in the lesions of Crohn's disease, are less common in the lesions of lichen nitidus.[82]
Endoscopy
A colonoscopy is the best test for making the diagnosis of Crohn's disease, as it allows direct visualization of the colon and the terminal ileum, identifying the pattern of disease involvement. On occasion, the colonoscope can travel past the terminal ileum, but it varies from patient to patient. During the procedure, the gastroenterologist can also perform a biopsy, taking small samples of tissue for laboratory analysis, which may help confirm a diagnosis. As 30% of Crohn's disease involves only the ileum,[1] cannulation of the terminal ileum is required in making the diagnosis. Finding a patchy distribution of disease, with involvement of the colon or ileum, but not the rectum, is suggestive of Crohn's disease, as are other endoscopic stigmata.[83] The utility of capsule endoscopy for this, however, is still uncertain. [84] A "cobblestone"-like appearance is seen in approximately 40% of cases of Crohn's disease upon colonoscopy, representing areas of ulceration separated by narrow areas of healthy tissue.
Radiologic tests
A small bowel follow-through may suggest the diagnosis of Crohn's disease and is useful when the disease involves only the small intestine. Because colonoscopy and gastroscopy allow direct visualization of only the terminal ileum and beginning of the duodenum, they cannot be used to evaluate the remainder of the small intestine. As a result, a barium follow-through X-ray, wherein barium sulfate suspension is ingested and fluoroscopic images of the bowel are taken over time, is useful for looking for inflammation and narrowing of the small bowel.[83][85] Barium enemas, in which barium is inserted into the rectum and fluoroscopy is used to image the bowel, are rarely used in the work-up of Crohn's disease due to the advent of colonoscopy. They remain useful for identifying anatomical abnormalities when strictures of the colon are too small for a colonoscope to pass through, or in the detection of colonic fistulae (in this case contrast should be performed with iodate substances).[86]
CT and MRI scans are useful for evaluating the small bowel with enteroclysis protocols.[87]They are also useful for looking for intra-abdominal complications of Crohn's disease, such as abscesses, small bowel obstructions, or fistulae.[88] Magnetic resonance imaging (MRI) is another option for imaging the small bowel as well as looking for complications, though it is more expensive and less readily available[89]
Nuclear scans
Multiphase white blood cell scans have been shown to be effective in detecting the locations of active Crohn's disease, particularly in hard to diagnose patients suffering with the early stages or a mild form of the disease with negative endoscopic and radiologic findings. The procedure, a type of nuclear medicine, uses white blood cells removed from the patient; they are tagged with a radioisotope, and then injected intravenously into the patient, and later scanned at several intervals to detect any abnormal white blood cell accumulation, such as pooling in the intestinal tract. Studies have also suggested such scans are useful to monitor the disease and evaluate the effectiveness of therapy.
Blood tests
A complete blood count may reveal anemia, which may be caused by blood loss, by vitamin B12 deficiency or, possibly, autoimmune hemolysis. The latter may be seen with ileitis because vitamin B12 is absorbed in the ileum.[90] Erythrocyte sedimentation rate, or ESR, and C-reactive protein measurements can also be useful to gauge the degree of inflammation.[91] It is also true in patients with an ilectomy done in response to the complication. Another cause of anemia is anemia of chronic disease, characterized by its microcytic and hypochromic anemia. There can be various reasons for it, including medication used in treatment of inflammatory bowel disease, like azathioprine, which can lead to cytopenia, and sulfasalazine, which can also result in folate malabsorption, etc. Testing for Saccharomyces cerevisiae antibodies (ASCA) and antineutrophil cytoplasmic antibodies (ANCA) has been evaluated to identify inflammatory diseases of the intestine[92] and to differentiate Crohn's disease from ulcerative colitis.[93] Furthermore, increasing amounts and levels of serological antibodies such as ASCA, antilaminaribioside [Glc(β1,3)Glb(β); ALCA], antichitobioside (GlcNAc(β1,4)GlcNAc(β); ACCA], antimannobioside [Man(α1,3)Man(α)AMCA], antiLaminarin [Glc(β1,3))3n(Glc(β1,6))n; anti-L] and antichitin [(GlcNAc(β1,4)n; anti-C] associate with disease behavior and surgery, and may aid in the prognosis of Crohn's disease.[94][95][96][97]
Comparison with ulcerative colitis
The most common disease that mimics the symptoms of Crohn's disease is ulcerative colitis, as both are inflammatory bowel diseases that can affect the colon with similar symptoms. It is important to differentiate these diseases, since the course of the diseases and treatments may be different. In some cases, however, it may not be possible to tell the difference, in which case the disease is classified as indeterminate colitis.[1][12][22]
Findings in diagnostic workup in Crohn's disease vs. ulcerative colitis
Sign Crohn's disease Ulcerative colitis Terminal ileum involvement Commonly Seldom Colon involvement Usually Always Rectum involvement Seldom Usually[42] Involvement around
the anusCommon[18] Seldom Bile duct involvement No increase in rate of primary sclerosing cholangitis Higher rate[98] Distribution of Disease Patchy areas of inflammation (Skip lesions) Continuous area of inflammation[42] Endoscopy Deep geographic and serpiginous (snake-like) ulcers Continuous ulcer Depth of inflammation May be transmural, deep into tissues[1][18] Shallow, mucosal Stenosis Common Seldom Granulomas on biopsy May have non-necrotizing non-peri-intestinal crypt granulomas[18][99][100] Non-peri-intestinal crypt granulomas not seen[42] Management
Main article: Management of Crohn's diseaseManagement in Crohn's disease vs. ulcerative colitis
Crohn's disease Ulcerative colitis Mesalazine less useful[101] More useful[101] Antibiotics Effective in long-term[102] Generally not useful[103] Surgery Often returns following
removal of affected partUsually cured by
removal of colonAt the present time, there is no cure for Crohn's disease and remission may not be possible or prolonged if achieved.[104] In cases where remission is possible, relapse can be prevented and symptoms controlled with medication, lifestyle changes, and, in some cases, surgery. Adequately controlled, Crohn's disease may not significantly restrict daily living.[105] Treatment for Crohn's disease is only when symptoms are active and involve first treating the acute problem, then maintaining remission.
Lifestyle changes
Certain lifestyle changes can reduce symptoms, including dietary adjustments Elemental diet, proper hydration, and smoking cessation. Smoking may increase Crohn's disease; stopping is recommended. Eating small meals frequently instead of big meals may also help with a low appetite. To manage symptoms have a balanced diet with proper portion control. Fatigue can be helped with regular exercise, a healthy diet, and enough sleep. A food diary may help with identifying foods that trigger symptoms. Some patients should follow a low dietary fiber diet to control symptoms especially if fibrous foods cause symptoms. Patients should avoid milk or dairy products as they have been shown in recent research (2007) to contribute to or even cause Crohn's disease.[105]
Medication
Acute treatment uses medications to treat any infection (normally antibiotics) and to reduce inflammation (normally aminosalicylate anti-inflammatory drugs and corticosteroids). When symptoms are in remission, treatment enters maintenance, with a goal of avoiding the recurrence of symptoms. Prolonged use of corticosteroids has significant side-effects; as a result, they are, in general, not used for long-term treatment. Alternatives include aminosalicylates alone, though only a minority are able to maintain the treatment, and many require immunosuppressive drugs.[18] It has been also suggested that antibiotics change the enteric flora, and their continuous use may pose the risk of overgrowth with pathogens such as Clostridium difficile.[106]
Medications used to treat the symptoms of Crohn's disease include 5-aminosalicylic acid (5-ASA) formulations, prednisone, immunomodulators such as azathioprine, mercaptopurine, methotrexate, infliximab, adalimumab,[22] certolizumab[107] and natalizumab.[108][109] Hydrocortisone should be used in severe attacks of Crohn's disease.[110]
Surgery
Crohn's cannot be cured by surgery, though it is used when partial or a full blockage of the intestine occurs. Surgery may also be required for complications such as obstructions, fistulas and/or abscesses, or if the disease does not respond to drugs. After the first surgery, Crohn's usually shows up at the site of the resection, however it can appear in other locations. After a resection, scar tissue builds up, which can cause strictures, which form when the intestines become too small to allow excrement to pass through easily, which can lead to a blockage. After the first resection, another resection may be necessary within five years.[111] For patients with an obstruction due to a stricture, two options for treatment are strictureplasty and resection of that portion of bowel. There is no statistical significance between strictureplasty alone versus strictureplasty and resection in cases of duodenal involvement. In these cases, re-operation rates were 31% and 27%, respectively, indicating that strictureplasty is a safe and effective treatment for selected patients with duodenal involvement.[112]
Short bowel syndrome (SBS, also short gut syndrome or simply short gut) can be caused by the surgical removal of the small intestines. It usually develops in those having had half or more of their small intestines removed.[113] Diarrhea is the main symptom of short bowel syndrome, however other symptoms may include cramping, bloating, and heartburn. Short bowel syndrome is treated with changes in diet, intravenous feeding, vitamin and mineral supplements, and treatment with medications. Another complication following surgery for Crohn's disease in which the terminal ileum has been removed is the development of excessive watery diarrhea. This is due to an inability of the ileum to reabsorb bile acids after resection of the terminal ileum.[citation needed]
In some cases of SBS, intestinal transplant surgery may be considered; though the number of transplant centres offering this procedure is quite small and it comes with a high risk due to the chance of infection and rejection of the transplanted intestine.[114]
Alternative medicine
More than half of people with Crohn's disease have tried complementary or alternative therapy.[115] These include diets, probiotics, fish oil and other herbal and nutritional supplements. The benefit of these medications is uncertain.[116][117]
- Acupuncture is used to treat inflammatory bowel disease in China, and is being used more frequently in Western society.[118] There is insufficient evidence to recommend the use of acupuncture, though further studies are warranted.[119]
- Homeopathy is frequently used in Germany as a treatment for Crohn's disease, though no clinical trials exist that demonstrate it is effective.[116]
Prognosis
Crohn's disease is a chronic condition for which there is currently no cure. It is characterised by periods of improvement followed by episodes when symptoms flare up. With treatment, most people achieve a healthy weight, and the mortality rate for the disease is relatively low. However, Crohn's disease is associated with an increased risk of small bowel and colorectal carcinoma, including bowel cancer.[120]
Epidemiology
The incidence of Crohn's disease has been ascertained from population studies in Norway and the United States and is similar at 6 to 7.1:100,000. The Crohn's and Colitis Foundation of America cites this number as approx 149:100,000; NIH cites 28 to 199 per 100,000.[121][122] Crohn's disease is more common in northern countries, and shows a higher preponderance in northern areas of the same country.[123] The incidence of Crohn's disease is thought to be similar in Europe but lower in Asia and Africa.[121] It also has a higher incidence in Ashkenazi Jews [22] and smokers.[124]
Crohn's disease has a bimodal distribution in incidence as a function of age: the disease tends to strike people in their teens and 20s, and people in their 50s through to their 70s, and ages in between due to not being diagnosed with Crohn's and being diagnosed instead with irritable bowel syndrome (IBS).[1][12] It is rarely diagnosed in early childhood. It usually strikes females who are pediatric patients more severely than males.[125] However, only slightly more women than men have Crohn's disease.[126] Parents, siblings or children of people with Crohn's disease are 3 to 20 times more likely to develop the disease.[127] Twin studies show a concordance of greater than 55% for Crohn's disease.[128]
History
Inflammatory bowel diseases were described by Giovanni Battista Morgagni (1682–1771) and by Scottish physician T. Kennedy Dalziel in 1913.[129]
Ileitis terminalis was first described by Polish surgeon Antoni Leśniowski in 1904, however, due to the precedence of Crohn's name in the alphabet, it became later to be known in the worldwide literature as Crohn’s disease.[citation needed] Only in Poland it continues to be named Leśniowski-Crohn’s disease. Burrill Bernard Crohn, an American gastroenterologist at New York City's Mount Sinai Hospital, described fourteen cases in 1932, and submitted them to the American Medical Association under the rubric of "Terminal ileitis: A new clinical entity". Later that year, he, along with colleagues Leon Ginzburg and Gordon Oppenheimer published the case series as "Regional ileitis: a pathologic and clinical entity".[14]
Research
Researchers at University College London have questioned the wisdom of suppressing the immune system in Crohn's, as the problem may be an underactive rather than an overactive immune system: Their study found that Crohn's patients showed an abnormally low response to an introduced infection, marked by a poor flow of blood to the wound, and the response improved when the patients were given sildenafil citrate.[46]
Recent studies using helminthic therapy or hookworms to treat Crohn's Disease and other (non-viral) auto-immune diseases seem to yield promising results.[130]
Numerous preclinical studies demonstrate that activation of the CB1 and CB2 cannabinoid receptors exert biological functions on the gastrointestinal tract.[131] Activation of CB1 and CB2 receptors in animals has shown a strong anti-inflammatory effect.[132] Cannabinoids and/or modulation of the endocannabinoid system is a novel therapeutic means for the treatment of numerous GI disorders, including inflammatory bowel diseases like Crohn's disease.[133]
- Methotrexate is a folate anti-metabolite drug that is also used for chemotherapy. It is useful in maintenance of remission for those no longer taking corticosteroids.[134]
- Metronidazole and ciprofloxacin are antibiotics used to treat Crohn's that have colonic or perianal involvement, although, in the United States, this use has not been approved by the Food and Drug Administration.[135] They are also used for treatment of complications, including abscesses and other infections accompanying Crohn's disease.[12]
- Thalidomide has shown response in reversing endoscopic evidence of disease.[136]
- Cannabis-derived drugs may be used to treat Crohn's Disease with their anti-inflammatory properties. Cannabis-derived drugs may also help to heal the gut lining.[137]
Notable cases
Main article: List of people diagnosed with Crohn's diseaseReferences
- ^ a b c d e f g h i j k l m n o Baumgart DC, Sandborn WJ (12 May 2007). "Inflammatory bowel disease: clinical aspects and established and evolving therapies.". The Lancet 369 (9573): 1641–57. doi:10.1016/S0140-6736(07)60751-X. PMID 17499606.
- ^ Mayo Clinic: Crohn's Disease
- ^ National Digestive Diseases Information Clearinghouse
- ^ Cho, JH; Brant, SR (2011 May). "Recent insights into the genetics of inflammatory bowel disease.". Gastroenterology 140 (6): 1704-12. PMID 21530736.
- ^ a b Dessein, R; Chamaillard, M, Danese, S (2008 Sep). "Innate immunity in Crohn's disease: the reverse side of the medal.". Journal of clinical gastroenterology 42 Suppl 3 Pt 1: S144-7. PMID 18806708.
- ^ Stefanelli, T; Malesci, A, Repici, A, Vetrano, S, Danese, S (2008 May). "New insights into inflammatory bowel disease pathophysiology: paving the way for novel therapeutic targets.". Current drug targets 9 (5): 413-8. PMID 18473770.
- ^ Marks, DJ; Rahman, FZ, Sewell, GW, Segal, AW (2010 Feb). "Crohn's disease: an immune deficiency state.". Clinical reviews in allergy & immunology 38 (1): 20-31. PMID 19437144.
- ^ Barrett, JC et al.; Hansoul, S; Nicolae, DL; Cho, JH; Duerr, RH; Rioux, JD; Brant, SR; Silverberg, MS et al. (August 2008). "Genome-wide association defines more than thirty distinct susceptibility loci for Crohn's disease". Nature Genetics 40 (8): 955–962. doi:10.1038/ng.175. PMC 2574810. PMID 18587394. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2574810.
- ^ a b Cosnes J (June 2004). "Tobacco and IBD: relevance in the understanding of disease mechanisms and clinical practice". Best Pract Res Clin Gastroenterol 18 (3): 481–96. doi:10.1016/j.bpg.2003.12.003. PMID 15157822.
- ^ Loftus, E.V.; P. Schoenfeld, W. J. Sandborn (January 2002). "The epidemiology and natural history of Crohn's disease in population-based patient cohorts from North America: a systematic review". Alimentary Pharmacology & Therapeutics 16 (1): 51–60. doi:10.1046/j.1365-2036.2002.01140.x. PMID 11856078.
- ^ a b Bernstein, Charles N.; Wajda, A; Svenson, LW; Mackenzie, A; Koehoorn, M; Jackson, M; Fedorak, R; Israel, D et al. (July 2006). "The epidemiology of inflammatory bowel disease in Canada: a population-based study". The American Journal of Gastroenterology 101 (7): 1559–68. doi:10.1111/j.1572-0241.2006.00603.x. PMID 16863561.
- ^ a b c d e f g h i Wu, George Y; Marcy L Coash, Senthil Nachimuthu (March 17, 2010). "Crohn Disease". eMedicine. http://emedicine.medscape.com/article/172940-overview. Retrieved 2010-04-15.
- ^ Le, Tri H (March 17, 2010). "Ulcerative colitis". eMedicine. http://emedicine.medscape.com/article/183084-overview. Retrieved 2010-04-15.
- ^ a b c Crohn BB, Ginzburg L, Oppenheimer GD (2000). "Regional ileitis: a pathologic and clinical entity. 1932". Mt. Sinai J. Med. 67 (3): 263–8. PMID 10828911.
- ^ a b Gasche C, Scholmerich J, Brynskov J, D'Haens G, Hanauer S, Irvine E, Jewell D, Rachmilewitz D, Sachar D, Sandborn W, Sutherland L (2000). "A simple classification of Crohn's disease: report of the Working Party for the World Congresses of Gastroenterology, Vienna 1998". Inflamm Bowel Dis 6 (1): 8–15. doi:10.1002/ibd.3780060103. PMID 10701144.
- ^ Dubinsky MC, Fleshner PP. (2003). "Treatment of Crohn's Disease of Inflammatory, Stenotic, and Fistulizing Phenotypes". Curr Treat Options Gastroenterol 6 (3): 183–200. doi:10.1007/s11938-003-0001-1. PMID 12744819.
- ^ a b c d e f internetmedicin.se > Inflammatorisk tarmsjukdom, kronisk, IBD By Robert Löfberg. Retrieved Oct 2010 Translate.
- ^ a b c d e Hanauer, Stephen B.; William Sandborn (2001-03-01). "Management of Crohn's disease in adults" (PDF). American Journal of Gastroenterology 96 (3): 635–43. doi:10.1111/j.1572-0241.2001.03671.x. PMID 11280528. http://www.acg.gi.org/physicians/guidelines/CrohnsDiseaseinAdults.pdf. Retrieved 2009-11-07.
- ^ a b Pimentel, Mark; Michael Chang, Evelyn J. Chow, Siamak Tabibzadeh, Viorelia Kirit-Kiriak, Stephan R. Targan, Henry C. Lin (2000). "Identification of a prodromal period in Crohn's disease but not ulcerative colitis". American Journal of Gastroenterology 95 (12): 3458–62. doi:10.1111/j.1572-0241.2000.03361.x. PMID 11151877.
- ^ Crohn's Disease Overview
- ^ a b Zieve, David; George F Longstreth (October 18, 2009). "Crohn's Disease". ADAM Health Illustrated Encyclopedia. http://www.healthline.com/adamcontent/crohns-disease. Retrieved 2010-08-16.
- ^ a b c d Podolsky, Daniel K. (2002). "Inflammatory bowel disease". New England Journal of Medicine 346 (6): 417–29. doi:10.1056/NEJMra020831. PMID 12167685. http://content.nejm.org/cgi/content/extract/347/6/417. Retrieved 2006-07-02.
- ^ Mueller, M. H.; M. E. Kreis, M. L. Gross, H. D. Becker, T. T. Zittel & E. C. Jehle (2002). "Anorectal functional disorders in the absence of anorectal inflammation in patients with Crohn's disease". British Journal of Surgery 89 (8): 1027–31. doi:10.1046/j.1365-2168.2002.02173.x. PMID 12153630.
- ^ Kumar, Vinay; Abul K. Abbas, Nelson Fausto (July 30, 2004). "Ch 17: The Gastrointestinal Tract". Robbins and Cotran: Pathologic Basis of Disease (7th ed.). Philadelphia, Pennsylvania: Elsevier Saunders. pp. 847. ISBN 0-7216-0187-1.
- ^ Taylor B, Williams G, Hughes L, Rhodes J (1989). "The histology of anal skin tags in Crohn's disease: an aid to confirmation of the diagnosis". Int J Colorectal Dis 4 (3): 197–9. doi:10.1007/BF01649703. PMID 2769004.
- ^ Fix, Oren K.; Jorge A. Soto, Charles W. Andrews and Francis A. Farraye (2004). "Gastroduodenal Crohn's disease". Gastrointestinel Endoscopy 60 (6): 985. doi:10.1016/S0016-5107(04)02200-X. PMID 15605018.
- ^ a b Beattie, R.M.; N. M. Croft, J. M. Fell, N. A. Afzal and R. B. Heuschkel (2006). "Inflammatory bowel disease". Archives of Disease in Childhood 91 (5): 426–32. doi:10.1136/adc.2005.080481. PMC 2082730. PMID 16632672. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2082730.
- ^ Büller, H.A. (1997). "Problems in diagnosis of IBD in children". The Netherlands Journal of Medicine 50 (2): S8–S11. doi:10.1016/S0300-2977(96)00064-2. PMID 9050326.
- ^ O'Keefe, S. J. (1996). "Nutrition and gastrointestinal disease". Scandinavian Journal of Gastroenterology Supplement 31 (220): 52–9. doi:10.3109/00365529609094750. PMID 8898436.
- ^ Danese, Silvio; Stefano Semeraro, Alfredo Papa, Italia Roberto, Franco Scaldaferri, Giuseppe Fedeli, Giovanni Gasbarrini, Antonio Gasbarrini (2005). "Extraintestinal manifestations in inflammatory bowel disease". World Journal of Gastroenterology 11 (46): 7227–36. PMID 16437620. http://www.wjgnet.com/1007-9327/11/7227.asp. Retrieved 2009-11-07.
- ^ a b Crohn's disease. professionals.epilepsy.com. Retrieved on July 13, 2007.
- ^ MedlinePlus Encyclopedia Small bowel bacterial overgrowth
- ^ Zadik Y, Drucker S, Pallmon S (Aug 2011). "Migratory stomatitis (ectopic geographic tongue) on the floor of the mouth". J Am Acad Dermatol 65 (2): 459–60. doi:10.1016/j.jaad.2010.04.016. PMID 21763590. http://www.sciencedirect.com/science/article/pii/S0190962210004883.
- ^ Prevalence defined as at least 5 health care contacts in a 10 year period for the condition, according to: Greenstein, A. J.; Janowitz, H. D.; Sachar, D. B. (1976). "The extra-intestinal complications of Crohn's disease and ulcerative colitis: a study of 700 patients". Medicine 55 (5): 401–412. doi:10.1097/00005792-197609000-00004. PMID 957999.
- ^ http://emedicine.medscape.com/article/442000-overview
- ^ Ekbom A, Helmick C, Zack M, Adami H (1990). "Increased risk of large-bowel cancer in Crohn's disease with colonic involvement". Lancet 336 (8711): 357–9. doi:10.1016/0140-6736(90)91889-I. PMID 1975343.
- ^ Collins P, Mpofu C, Watson A, Rhodes J (2006). Watson, Alastair J. ed. "Strategies for detecting colon cancer and/or dysplasia in patients with inflammatory bowel disease". Cochrane Database Syst Rev (2): CD000279. doi:10.1002/14651858.CD000279.pub3. PMID 16625534.
- ^ Lynne V McFarland (2008). "Colorectal cancer and dysplasia in inflammatory bowel disease". World Journal of Gastroenterology: 2665.
- ^ Evans J, Steinhart A, Cohen Z, McLeod R (2003). "Home total parenteral nutrition: an alternative to early surgery for complicated inflammatory bowel disease". J Gastrointest Surg 7 (4): 562–6. doi:10.1016/S1091-255X(02)00132-4. PMID 12763417.
- ^ "Complications of Crohn's Disease". Centocor Ortho Biotech. https://www.livingwithcrohnsdisease.com/livingwithcrohnsdisease/crohns_disease/complications_of_crohns.html. Retrieved 2009-11-07.
- ^ Kaplan, C (2005-10-21). "IBD and Pregnancy: What You Need to Know". Crohn's and Colitis Foundation of America. http://www.ccfa.org/about/news/pregnancy. Retrieved 2009-11-07.
- ^ a b c d Kornbluth, Asher; David B. Sachar (July 2004). "Ulcerative colitis practice guidelines in adults (update): American College of Gastroenterology, Practice Parameters Committee" (PDF). American Journal of Gastroenterology 99 (7): 1371–85. doi:10.1111/j.1572-0241.2004.40036.x. PMID 15233681. Archived from the original on April 6, 2008. http://web.archive.org/web/20080406030552/http://www.acg.gi.org/physicians/guidelines/UlcerativeColitisUpdate.pdf. Retrieved 2009-11-07.
- ^ Crohn's Disease Overview
- ^ Braat H, Peppelenbosch MP, Hommes DW (August 2006). "Immunology of Crohn's disease". Ann. N. Y. Acad. Sci. 1072: 135–54. doi:10.1196/annals.1326.039. PMID 17057196.
- ^ Henckaerts L, Figueroa C, Vermeire S, Sans M (May 2008). "The role of genetics in inflammatory bowel disease". Curr Drug Targets 9 (5): 361–8. doi:10.2174/138945008784221161. PMID 18473763.
- ^ a b c Marks DJ, Harbord MW, MacAllister R, Rahman FZ, Young J, Al-Lazikani B, Lees W, Novelli M, Bloom S, Segal AW (2006). "Defective acute inflammation in Crohn's disease: a clinical investigation". Lancet 367 (9511): 668–78. doi:10.1016/S0140-6736(06)68265-2. PMC 2092405. PMID 16503465. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2092405.
- ^ Comalada M, Peppelenbosch MP (September 2006). "Impaired innate immunity in Crohn's disease". Trends Mol Med 12 (9): 397–9. doi:10.1016/j.molmed.2006.07.005. PMID 16890491.
- ^ "Crohn's disease has strong genetic link: study". Crohn's and Colitis Foundation of America. 2007-04-16. http://www.ccfa.org/reuters/geneticlink. Retrieved 2009-11-07.
- ^ Ogura Y, Bonen DK, Inohara N, et al. (2001). "A frameshift mutation in NOD2 associated with susceptibility to Crohn's disease". Nature 411 (6837): 603–6. doi:10.1038/35079114. PMID 11385577.
- ^ Cuthbert A, Fisher S, Mirza M, et al. (2002). "The contribution of NOD2 gene mutations to the risk and site of disease in inflammatory bowel disease". Gastroenterology 122 (4): 867–74. doi:10.1053/gast.2002.32415. PMID 11910337.
- ^ Kaser, A; Lee, AH; Franke, A; Glickman, JN; Zeissig, S; Tilg, H; Nieuwenhuis, EE; Higgins, DE et al. (5 September 2008). "XBP1 links ER stress to intestinal inflammation and confers genetic risk for human inflammatory bowel disease". Cell (Cell Press) 134 (5): 743–756. doi:10.1016/j.cell.2008.07.021. PMC 2586148. PMID 18775308. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2586148.
- ^ Clevers, H (2009). "Inflammatory Bowel Disease, Stress, and the Endoplasmic Reticulum". N Engl J Med 360 (7): 726–727. doi:10.1056/NEJMcibr0809591. PMID 19213688.
- ^ a b R Shoda, K Matsueda, S Yamato and N Umeda (1996). "Epidemiologic analysis of Crohn disease in Japan: increased dietary intake of n-6 polyunsaturated fatty acids and animal protein relates to the increased incidence of Crohn disease in Japan". American Journal of Clinical Nutrition (The American Society for Clinical Nutrition) 64 (5): 741–745. PMID 8615358.
- ^ Lesko S, Kaufman D, Rosenberg L, et al. (1985). "Evidence for an increased risk of Crohn's disease in oral contraceptive users". Gastroenterology 89 (5): 1046–9. PMID 4043662.
- ^ Reddy D, Siegel CA, Sands BE, Kane S (July 2006). "Possible association between isotretinoin and inflammatory bowel disease". The American journal of gastroenterology 101 (7): 1569–73. doi:10.1111/j.1572-0241.2006.00632.x. PMID 16863562.
- ^ Borobio E, Arín A, Valcayo A, Iñarrairaegui M, Nantes O, Prieto C (2004). "[Isotretinoin and ulcerous colitis]" (in Spanish; Castilian). An Sist Sanit Navar 27 (2): 241–3. PMID 15381956.
- ^ Reniers DE, Howard JM (October 2001). "Isotretinoin-induced inflammatory bowel disease in an adolescent". Ann Pharmacother 35 (10): 1214–6. doi:10.1345/aph.10368. PMID 11675849. http://www.theannals.com/cgi/pmidlookup?view=long&pmid=11675849.
- ^ Crohn's and Colitis Foundation of America About Crohn's. Retrieved on: 2011-09-30.
- ^ Cobrin GM, Abreu MT (2005). "Defects in mucosal immunity leading to Crohn's disease". Immunol. Rev. 206: 277–95. doi:10.1111/j.0105-2896.2005.00293.x. PMID 16048555.
- ^ a b Elson, CO; Cong, Y; Weaver, CT; Schoeb, TR; Mcclanahan, TK; Fick, RB; Kastelein, RA (2007). "Monoclonal Anti–Interleukin 23 Reverses Active Colitis in a T Cell–Mediated Model in Mice". Gastroenterology 132 (7): 2359–70. doi:10.1053/j.gastro.2007.03.104. PMID 17570211.
- ^ Prescott NJ, Fisher SA, Franke A, et al. (2007). "A nonsynonymous SNP in ATG16L1 predisposes to ileal Crohn's disease and is independent of CARD15 and IBD5". Gastroenterology 132 (5): 1665–71. doi:10.1053/j.gastro.2007.03.034. PMID 17484864.
- ^ Marks DJ, Segal AW. (January 2008). "Innate immunity in inflammatory bowel disease: a disease hypothesis". J Pathol. 214 (2): 260–6. doi:10.1002/path.2291. PMC 2635948. PMID 18161747. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2635948.
- ^ Dessein R, Chamaillard M, Danese S (September 2008). "Innate immunity in Crohn's disease: the reverse side of the medal". J Clin Gastroenterol 42 (Suppl 3 Pt 1): S144–7. doi:10.1097/MCG.0b013e3181662c90. PMID 18806708.
- ^ "OVERVIEW: MAP and Crohn's Disease Research". Paratuberculosis Awareness & Research Association. http://www.crohns.org/research/index.htm. Retrieved 2009-11-07.
- ^ Sartor, R. (July 2006). "Mechanisms of Disease: pathogenesis of Crohn's disease and ulcerative colitis". Nature Clinical Practice Gastroenterology & Hepatology 3 (7): 390–407. doi:10.1038/ncpgasthep0528. PMID 16819502. http://www.nature.com/nrgastro/journal/v3/n7/full/ncpgasthep0528.html.
- ^ Naser SA, Collins MT (2005). "Debate on the lack of evidence of Mycobacterium avium subsp. paratuberculosis in Crohn's disease". Inflamm. Bowel Dis. 11 (12): 1123. doi:10.1097/01.MIB.0000191609.20713.ea. PMID 16306778.
- ^ Giaffer MH, Clark A, Holdsworth CD (1992). "Antibodies to Saccharomyces cerevisiae in patients with Crohn's disease and their possible pathogenic importance". Gut 33 (8): 1071–5. doi:10.1136/gut.33.8.1071. PMC 1379444. PMID 1398231. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1379444.
- ^ Baumgart M et al. (2007). "Culture independent analysis of ileal mucosa reveals a selective increase in invasive Escherichia coli of novel phylogeny relative to depletion of Clostridiales in Crohn's disease involving the ileum". The ISME Journal 1 (5): 403–18. doi:10.1038/ismej.2007.52. PMID 18043660. http://www.nature.com/ismej/journal/v1/n5/full/ismej200752a.html.
- ^ "Possible links between Crohn’s disease and Paratuberculosis" (PDF). EUROPEAN COMMISSION DIRECTORATE-GENERAL HEALTH & CONSUMER PROTECTION. http://ec.europa.eu/food/fs/sc/scah/out38_en.pdf. Retrieved 2009-11-07.
- ^ Gui GP, Thomas PR, Tizard ML, Lake J, Sanderson JD, Hermon-Taylor J (March 1997). "Two-year-outcomes analysis of Crohn's disease treated with rifabutin and macrolide antibiotics" (PDF). J. Antimicrob. Chemother. 39 (3): 393–400. doi:10.1093/jac/39.3.393. PMID 9096189. http://jac.oxfordjournals.org/cgi/reprint/39/3/393.
- ^ Cenac N, Andrews CN, Holzhausen M, et al. (March 2007). "Role for protease activity in visceral pain in irritable bowel syndrome". J. Clin. Invest. 117 (3): 636–47. doi:10.1172/JCI29255. PMC 1794118. PMID 17304351. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1794118.
- ^ Cenac N, Coelho AM, Nguyen C, et al. (November 2002). "Induction of Intestinal Inflammation in Mouse by Activation of Proteinase-Activated Receptor-2". Am. J. Pathol. 161 (5): 1903–15. doi:10.1016/S0002-9440(10)64466-5. PMC 1850779. PMID 12414536. http://ajp.amjpathol.org/cgi/pmidlookup?view=long&pmid=12414536.
- ^ Boorom KF, Smith H, Nimri L, et al. (October 2008). "Oh my aching gut: irritable bowel syndrome, Blastocystis, and asymptomatic infection". Parasit Vectors 1 (1): 40. doi:10.1186/1756-3305-1-40. PMC 2627840. PMID 18937874. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2627840.
- ^ Hugot, Jean-Pierre; Alberti, Corinne; Berrebi, Dominique; Bingen, Edouard; Cezard, Jean-Pierre (2003-12-13). "Crohn's disease: the cold chain hypothesis". The Lancet 362 (9400): 2012–2015. doi:10.1016/S0140-6736(03)15024-6. http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(03)15024-6.
- ^ "Fridges blamed for Crohn's disease rise". Medical News TODAY. 2003-12-12. http://www.medicalnewstoday.com/articles/4849.php.
- ^ Forbes, Alastair; Kalantzis, Tommy (July 2006). "Crohn's disease : the cold chain hypothesis". International Journal of Colorectal Disease (Springer Berlin / Heidelberg) 21 (5): 399–401. doi:10.1007/s00384-005-0003-7. ISSN 0179-1958. PMID 16059694. http://www.springerlink.com/content/p6q21tp76x013u51/. Retrieved 2009-11-04.
- ^ Subramanian, Sreedhar; Carol, L. Roberts; Hart, C. Anthony; Martin, Helen M.; Edwards, Steve W.; Rhodes, Jonathan M.; Campbell, Barry J. (2008). "Replication of Colonic Crohn's Disease Mucosal Escherichia coli Isolates within Macrophages and Their Susceptibility to Antibiotics". Antimicrobial Agents and Chemotherapy 52 (2): 427–434. doi:10.1128/AAC.00375-07. PMC 2224732. PMID 18070962. http://aac.asm.org/cgi/content/abstract/52/2/427.
- ^ Mpofu, Chiedzo M.; Cambell, Barry J.; Subramanin, Sreedhar; Marshall-Clarke, Stuart; Hart, Anthony C.; Cross, Andy; Roberts, Carol L.; McGoldrick, Adrian et al. (2007). "Microbial Mannan Inhibits Bacterial Killing by Macrophages: A Possible Pathogenic Mechanism for Crohn's Disease". Gastroenterology, the official journal of the AGA Institute 133 (5): 1487–1498. doi:10.1053/j.gastro.2007.08.004. PMID 17919633. http://www.gastrojournal.org/article/S0016-5085(07)01450-3/abstract.
- ^ "New insights into Crohn's Disease". http://www.liv.ac.uk/researchintelligence/issue33/crohns.htm.
- ^ Crawford JM. "The Gastrointestinal tract, Chapter 17". In Cotran RS, Kumar V, Robbins SL. Robbins Pathologic Basis of Disease: 5th Edition. W.B. Saunders and Company, Philadelphia, 1994.
- ^ HCP: Pill Cam, Capsule Endoscopy, Esophageal Endoscopy
- ^ Scheinfeld NS, Teplitz E, McClain SA (November 2001). "Crohn's disease and lichen nitidus: a case report and comparison of common histopathologic features". Inflammatory bowel diseases 7 (4): 314–8. doi:10.1097/00054725-200111000-00006. PMID 11720321.
- ^ a b Hara, Amy K.; Jonathan A. Leighton, Russell I. Heigh, Virender K. Sharma, Alvin C. Silva, Giovanni De Petris, Joseph G. Hentz and David E. Fleischer (January 2006). "Crohn disease of the small bowel: preliminary comparison among CT enterography, capsule endoscopy, small-bowel follow-through, and ileoscopy". Radiology 238 (1): 128–34. doi:10.1148/radiol.2381050296. PMID 16373764.
- ^ Triester, Stuart L.; Jonathan A. Leighton, Grigoris I. Leontiadis, Suryakanth R. Gurudu, David E. Fleischer, Amy K. Hara, Russell I. Heigh, Arthur D. Shiff, and Virender K. Sharma (2006). "A meta-analysis of the yield of capsule endoscopy compared to other diagnostic modalities in patients with non-stricturing small bowel Crohn's disease". The American Journal of Gastroenterology 101 (5): 954–64. doi:10.1111/j.1572-0241.2006.00506.x. PMID 16696781.
- ^ Dixon, P.M.; M.E. Roulston and D.J. Nolan (1993). "The small bowel enema: a ten year review". Clinical Radiology 47 (1): 46–8. doi:10.1016/S0009-9260(05)81213-9. PMID 8428417.
- ^ Carucci, L. R.; M. S. Levine (2002). "Radiographic imaging of inflammatory bowel disease". Gastroenterology Clinics of North America 31 (1): 93–117. doi:10.1016/S0889-8553(01)00007-3. PMID 12122746.
- ^ Rajesh, A.; D.D.T. Maglinte (2006). "Multislice CT enteroclysis: technique and clinical applications". Clinical Radiology 61 (1): 31–9. doi:10.1016/j.crad.2005.08.006. PMID 16356814.
- ^ Zissin, Rivka; Marjorie Hertz, Alexandra Osadchy, Ben Novis and Gabriela Gayer (2005). "Computed Tomographic Findings of Abdominal Complications of Crohn's Disease—Pictorial Essay" (PDF). Canadian Association of Radiologists Journal 56 (1): 25–35. PMID 15835588. Archived from the original on April 6, 2008. http://web.archive.org/web/20080406030552/http://www.carj.ca/issues/2005-Feb/25/pg25.pdf. Retrieved 2009-11-07.
- ^ MacKalski, B. A.; C. N. Bernstein (2005). "New diagnostic imaging tools for inflammatory bowel disease". Gut 55 (5): 733–41. doi:10.1136/gut.2005.076612. PMC 1856109. PMID 16609136. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1856109.
- ^ Goh, Jason; C. A. O'Morain (2003). "Review article: nutrition and adult inflammatory bowel disease". Alimentary Pharmacology & Therapeutics 17 (3): 307–20. doi:10.1046/j.1365-2036.2003.01482.x. PMID 12562443.
- ^ Chamouard, Patrick; Zoe Richert, Nicolas Meyer, Gabriel Rahmi, René Baumann (2006). "Diagnostic Value of C-Reactive Protein for Predicting Activity Level of Crohn's Disease". Clinical Gastroenterology and Hepatology 4 (7): 882–7. doi:10.1016/j.cgh.2006.02.003. PMID 16630759. Epub ahead of print
- ^ Kaila, B; K Orr and C N Bernstein (2005). "The anti-Saccharomyces cerevisiae antibody assay in a province-wide practice: accurate in identifying cases of Crohn's disease and predicting inflammatory disease". The Canadian Journal of Gastroenterology 19 (12): 717–21. PMID 16341311. http://www.pulsus.com/journals/abstract.jsp?sCurrPg=journal&jnlKy=2&atlKy=743&isuKy=263&isArt=t. Retrieved 2006-07-02.
- ^ Israeli, E.; I. Grotto, B. Gilburd, R. D. Balicer, E. Goldin, A. Wiik and Y. Shoenfeld (2005). "Anti-Saccharomyces cerevisiae and antineutrophil cytoplasmic antibodies as predictors of inflammatory bowel disease". Gut 54 (9): 1232–6. doi:10.1136/gut.2004.060228. PMC 1774672. PMID 16099791. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1774672.
- ^ Ferrante, M.; L. Henckaerts, M. Joossens, M. Pierik, S. Joossens, N. Dotan, G.L. Norman , R.T. Altstock , K. Van Steen , P. Rutgeerts , G. Van Assche and S.Vermeire (2007). "New serological markers in inflammatory bowel disease are associated with complicated disease behaviour". Gut 56 (10): 1394–403. doi:10.1136/gut.2006.108043. PMC 2000264. PMID 17456509. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2000264.
- ^ Papp, M.; I. Altorjay, N. Dotan, K. Palatka, I. Foldi, J. Tumpek, S. Sipka, M. Udvardy, T. Dinya, L. Lakatos, A. Kovacs, T. Molnar, Z. Tulassay, P. Mihelle, G.L. Norman, T. Szamosi , J. Papp; Hungarian IBD Study Group and P.L. Lakatos (2008). "New serological markers for inflammatory bowel disease are associated with earlier age at onset, complicated disease behavior, risk for surgery, and NOD2/CARD15 genotype in a Hungarian IBD cohort". Am J Gastroenterol 104 (6): 1426–34. doi:10.1111/j.1572-0241.2007.01652.x. PMID 18047543.
- ^ Seow, C.H.; J.M. Stempak, W. Xu, H. Lan, A.M. Griffiths, G.R. Greenberg, A.H. Steinhart, N. Dotan and M.S. Silverberg (2009). "Novel anti-glycan antibodies related to inflammatory bowel disease diagnosis and phenotype". Am J Gastroenterol 104 (6): 1426–34. doi:10.1038/ajg.2009.79. PMID 19491856.
- ^ Dotan, I. (2007). "Serologic markers in inflammatory bowel disease: tools for better diagnosis and disease stratification". Expert Rev Gastroenterol Hepatol 1 (2): 265–74. doi:10.1586/17474124.1.2.265. PMID 19072419.
- ^ Broomé, Ulrika; Annika Bergquist (February 2006). "Primary sclerosing cholangitis, inflammatory bowel disease, and colon cancer". Seminars in Liver Disease 26 (1): 31–41. doi:10.1055/s-2006-933561. PMID 16496231.
- ^ Shepherd, NA. (August 2002). "Granulomas in the diagnosis of intestinal Crohn's disease: a myth exploded?". Histopathology 41 (2): 166–8. doi:10.1046/j.1365-2559.2002.01441.x. PMID 12147095.
- ^ Mahadeva, U.; Martin, JP.; Patel, NK.; Price, AB. (July 2002). "Granulomatous ulcerative colitis: a re-appraisal of the mucosal granuloma in the distinction of Crohn's disease from ulcerative colitis.". Histopathology 41 (1): 50–5. doi:10.1046/j.1365-2559.2002.01416.x. PMID 12121237.
- ^ a b Pages 152-156 (Section: Inflammatory bowel disease(IBD)) in:Elizabeth D Agabegi; Agabegi, Steven S. (2008). Step-Up to Medicine (Step-Up Series). Hagerstwon, MD: Lippincott Williams & Wilkins. ISBN 0-7817-7153-6.
- ^ Feller, M.; Huwiler, K.; Schoepfer, A.; Shang, A.; Furrer, H.; Egger, M. (2010). "Long-term antibiotic treatment for Crohn's disease: systematic review and meta-analysis of placebo-controlled trials". Clinical Infectious Diseases 50 (4): 473–480. doi:10.1086/649923. PMID 20067425.
- ^ [1] Section "Antibiotics and Ulcerative Colitis" in: Prantera, C.; Scribano, M. (2009). "Antibiotics and probiotics in inflammatory bowel disease: why, when, and how". Current opinion in gastroenterology 25 (4): 329–333. doi:10.1097/MOG.0b013e32832b20bf. PMID 19444096.
- ^ "Clinical Research Alliance Update" (PDF). Crohn's and Colitis Foundation of America. 2007-05-01. http://www.ccfa.org/ccfaprof/research-grant-opps/documents/May-2007-Newsletter.pdf. Retrieved 2008-02-14.
- ^ a b Fries, WS; Nazario, B (2007-05-16). "Crohn's Disease: 54 Tips to Help You Manage". WebMD. http://www.webmd.com/digestive-disorders/features/crohns-disease-54-tips-to-help-you-manage. Retrieved 2008-02-14.
- ^ Shanahan, Fergus (2002). "Crohn's disease". The Lancet (Elsevier Science) 359 (9300): 67.
- ^ "FDA Approves Cimzia to Treat Crohn's Disease" (Press release). Food and Drug Administration. April 22, 2008. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2008/ucm116882.htm. Retrieved 2009-11-04.
- ^ Sandborn, W.J.; Colombel, J.F.; Enns, R.; Feagan, B.G.; Hanauer, S.B.; Lawrance, I.C.; Panaccione, R.; Sanders, M.; Schreiber, S.; Targan, S.; Others, (2005). "Natalizumab Induction and Maintenance Therapy for Crohn's Disease". New England Journal of Medicine 353 (18): 1912–25. doi:10.1056/NEJMoa043335. PMID 16267322.
- ^ Macdonald, JK; Mcdonald, JW; McDonald, J.W.D. (2006). MacDonald, John. ed. "Natalizumab for induction of remission in Crohn's disease (Cochrane Review)". The Cochrane Database of Systematic Reviews 3: 1465–858. doi:10.1002/14651858.CD006097. PMID 16856112. http://dellboy.update-software.com/abstracts/AB006097.htm. Retrieved 2008-02-15.[dead link]
- ^ Longmore, Murray; Ian Wilkinson, Tom Turmezei, Chee Kay Cheung (2007). Oxford Handbook of Clinicial Medicine, 7th edition. Oxford University Press. pp. 266–7. ISBN 0-19-856837-1.
- ^ Tresca, AJ (2007-01-12). "Resection Surgery for Crohn's Disease". About.com. http://ibdcrohns.about.com/od/surgeryprocedures/a/resectioncrohns.htm. Retrieved 2008-02-14.
- ^ Ozuner G, Fazio VW, Lavery IC, Milsom JW, Strong SA (1996). "Reoperative rates for Crohn's disease following strictureplasty. Long-term analysis". Dis. Colon Rectum 39 (11): 1199–203. doi:10.1007/BF02055108. PMID 8918424.
- ^ Short Bowel Syndrome as defined by the National Institute of Diabetes and Digestive and Kidney Diseases
- ^ Rhodes, M (2006-10-24). "Intestinal transplant for Crohn's disease". Everyday Health. http://www.revolutionhealth.com/conditions/digestive/crohns-disease/surgery/intestinal-transplant. Retrieved 2009-03-22.
- ^ Caprilli R, Gassull M, Escher J et al. (2006). "European evidence based consensus on the diagnosis and management of Crohn's disease: special situations". Gut 55 Suppl 1 (Suppl 1): i36–58. doi:10.1136/gut.2005.081950c. PMC 1859996. PMID 16481630. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1859996.
- ^ a b Smart, H.L.; J.F. Mayberry, M. Atkinson (1986). "Alternative medicine consultations and remedies in patients with the irritable bowel syndrome". Gut - an international journal of Gastroenterology and Hepatology 27 (7): 826–828. doi:10.1136/gut.27.7.826. http://gut.bmj.com/content/27/7/826.abstract. Retrieved 21 September 2010. "This study has shown that the use of alternative medicine is common in patients with irritable bowel syndrome and this does not appear to be explicable in terms of the nature, chronicity or refractoriness to treatment of symptoms."
- ^ "Use of complementary and alternative medicine in Germany – a survey of patients with inflammatory bowel disease". BioMed Central. http://www.biomedcentral.com/1472-6882/6/19. Retrieved 21 September 2010. "At the same time, further clinical studies assessing the most commonly used CAM therapies are urgently needed. Research in CAM offers the chance to discover new treatment options in the management of IBD but may also protect patients from ineffective and expensive 'pseudo'-therapies."
- ^ Joos S, Brinkhaus B, Maluche C, et al. (2004). "Acupuncture and moxibustion in the treatment of active Crohn's disease: a randomized controlled study". Digestion 69 (3): 131–9. doi:10.1159/000078151. PMID 15114043.
- ^ "The second European evidence-based Consensus on the diagnosis and management of Crohn's disease: Special situations". ScienceDirect. Journal of Crohn's and Colitis (2010) 4, 63-101. https://http://gut.bmj.com/content/55/suppl_1/i36.full.pdf. Retrieved 21 September 2010. "the colitis activity index fell significantly in the treatment group compared to the sham acupuncture group. However, recruitment did not reach its target and the number of patients was small."
- ^ a b Hiatt, Robert A.; Leon Kaufman (1988). "Epidemiology of inflammatory bowel disease in a defined northern California population". Western Journal of Medicine 149 (5): 541–6. PMC 1026530. PMID 3250100. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1026530.
- ^ Moum, B.; M. H. Vatn, A. Ekbom, E. Aadland, O. Fausa, I. Lygren, N. Stray, J. Sauar, T. Schulz (1996). "Incidence of Crohn's disease in four counties in southeastern Norway, 1990-93. A prospective population-based study. The Inflammatory Bowel South-Eastern Norway (IBSEN) Study Group of Gastroenterologists". Scandinavian Journal of Gastroenterology 31 (4): 355–61. doi:10.3109/00365529609006410. PMID 8726303.
- ^ Shivananda, S.; J. Lennard-Jones, R. Logan, N. Fear, A. Price, L. Carpenter and M. van Blankenstein (1996). "Incidence of inflammatory bowel disease across Europe: is there a difference between north and south? Results of the European Collaborative Study on Inflammatory Bowel Disease (EC-IBD)". Gut 39 (5): 690–7. doi:10.1136/gut.39.5.690. PMC 1383393. PMID 9014768. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1383393.
- ^ Effects of light smoking consumption on the clinical course of Crohn's disease. Seksik P, Nion-Larmurier I, Sokol H, Beaugerie L, Cosnes J. Inflamm Bowel Dis. 2009
- ^ "Crohn's disease manifests differently in boys and girls". Crohn's and Colitis Foundation of America. http://www.ccfa.org/reuters/ibdboysgirls.
- ^ "Who is affected by Crohn's disease". Healthwise. http://www.webmd.com/hw-popup/who-is-affected-by-crohns-disease.
- ^ Satsangi J, Jewell DP, Bell JI (1997). "The genetics of inflammatory bowel disease". Gut 40 (5): 572–4. PMC 1027155. PMID 9203931. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1027155.
- ^ Tysk C, Lindberg E, Järnerot G, Flodérus-Myrhed B (1988). "Ulcerative colitis and Crohn's disease in an unselected population of monozygotic and dizygotic twins. A study of heritability and the influence of smoking". Gut 29 (7): 990–6. doi:10.1136/gut.29.7.990. PMC 1433769. PMID 3396969. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1433769.
- ^ Kirsner JB (1988). "Historical aspects of inflammatory bowel disease". J. Clin. Gastroenterol. 10 (3): 286–97. doi:10.1097/00004836-198806000-00012. PMID 2980764.
- ^ Croese J, O'neil J, Masson J, et al. (2006). "A proof of concept study establishing Necator americanus in Crohn's patients and reservoir donors". Gut 55 (1): 136–7. doi:10.1136/gut.2005.079129. PMC 1856386. PMID 16344586. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1856386.
- ^ *Massa and Monory; Monory, K (2007). "Endocannabinoids and the gastrointestinal tract". Journal of Endocrinological Investigation 29 ((Suppl)): 47–57. PMID 16751708.
- ^ *Massa et al.; Storr, Martin; Lutz, Beat (2005). "The endocannabinoid system in the physiology and pathophysiology of the gastrointestinal tract". Journal of Molecular Medicine 12 (12): 944–54. doi:10.1007/s00109-005-0698-5. PMID 16133420.
- ^ *Izzo and Coutts.; Coutts, AA (2005). "Cannabinoids and the digestive tract". Handbook of Experimental Pharmacology (168): 573–98. PMID 16596788.
- ^ Feagan BG, Fedorak RN, Irvine EJ, et al. (2000). "A comparison of methotrexate with placebo for the maintenance of remission in Crohn's disease. North American Crohn's Study Group Investigators". N. Engl. J. Med. 342 (22): 1627–32. doi:10.1056/NEJM200006013422202. PMID 10833208.
- ^ Ursing B, Alm T, Bárány F, et al. (1982). "A comparative study of metronidazole and sulfasalazine for active Crohn's disease: the cooperative Crohn's disease study in Sweden. II. Result". Gastroenterology 83 (3): 550–62. PMID 6124474.
- ^ Cohen LB (2004). "Re: Disappearance of Crohn's ulcers in the terminal ileum after thalidomide therapy. Can J Gastroenterol 2004; 18(2): 101-104". Can. J. Gastroenterol. 18 (6): 419; author reply 419. PMID 15230268.
- ^ Wright, K; Rooney, N; Feeney, M; Tate, J; Robertson, D; Welham, M; Ward, S (2005). "Differential Expression of Cannabinoid Receptors in the Human Colon: Cannabinoids Promote Epithelial Wound Healing". Gastroenterology 129 (2): 437. doi:10.1053/j.gastro.2005.05.026. PMID 16083701.
External links
Inflammatory bowel disease: Crohn's disease and ulcerative colitis Main Anatomical terms Abdominal pain · Anal abscess · Erythema nodosum · Fistula · Granuloma · Ileum · Ileitis · Malabsorption · Proctitis · Protein losing enteropathy · Pyoderma gangrenosum · Sacroiliitis · Short bowel syndrome · Small bowel obstruction · StenosisHistory Organizations People List of people diagnosed with Crohn's disease · Deaths from Crohn's diseaseCategories:- Autoimmune diseases
- Noninfective enteritis and colitis
- Membrane transport protein disorders
- Inflammations
- Abdominal pain







Wikimedia Foundation. 2010.