- Cerebral arteriovenous malformation
-
Cerebral arteriovenous malformation Classification and external resources 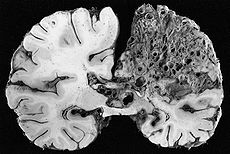
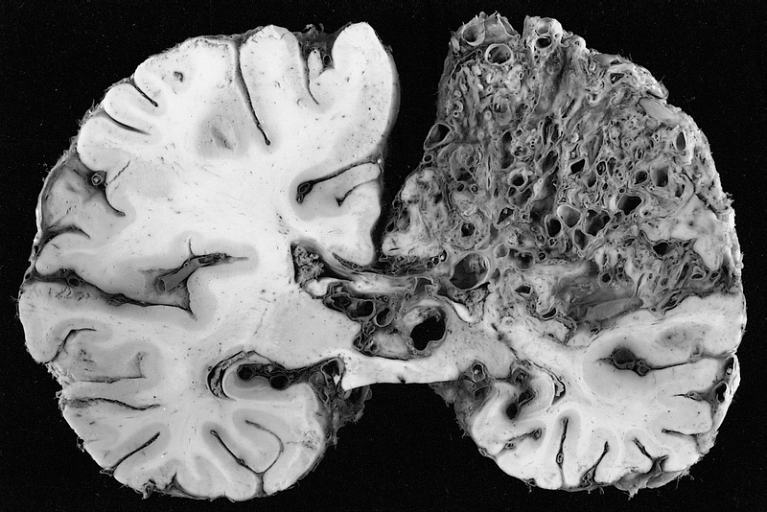
Large arteriovenous malformation of the parietal lobeICD-10 Q28.2 ICD-9 747.81 OMIM 108010 DiseasesDB 2224 MedlinePlus 000779 eMedicine neuro/21 article/252426 article/337220 MeSH D002538 A cerebral arteriovenous malformation (AVM) is an abnormal connection between the arteries and veins in the brain.
Contents
Signs and symptoms
The most frequently observed problems related to an AVM are headaches and seizures while at least 15% of the population at detection have no symptoms at all.[1] Other common symptoms are a pulsing noise in the head, progressive weakness and numbness and vision changes.[2][3]
In serious cases, the blood vessels rupture and there is bleeding within the brain (intracranial hemorrhage). Nevertheless in more than half of patients with AVM, hemorrhage is the first symptom.[3] Symptoms due to bleeding include loss of consciousness, sudden and severe headache, nausea, vomiting, incontinence, and blurred vision, amongst others.[2] Impairments caused by local brain tissue damage on the bleed site are also possible, including seizure, one-sided weakness (hemiparesis), a loss of touch sensation on one side of the body and deficits in language processing (aphasia).[2] Minor bleeding can occur with no noticeable symptoms.
AVMs in certain critical locations may stop the circulation of the cerebrospinal fluid, causing accumulation of the fluid within the skull and giving rise to a clinical condition called hydrocephalus.[3] A stiff neck can occur as the result of increased pressure within the skull and irritation of the meninges.
Diagnosis
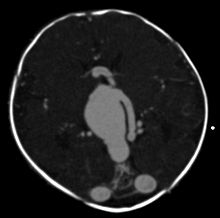 Axial image from computerized tomography angiogram showing arteriovenous communication in vein of Galen malformation
Axial image from computerized tomography angiogram showing arteriovenous communication in vein of Galen malformation
An AVM diagnosis is established by neuroimaging studies after a complete neurological and physical examination.[3][4] Three main techniques are used to visualize the brain and search for AVM: computed tomography (CT), magnetic resonance imaging (MRI), and cerebral angiography.[4] A CT scan of the head is usually performed first when the subject is symptomatic. It can suggest the approximate site of the bleed.[1] MRI is more sensitive than CT in the diagnosis of AVMs and provides better information about the exact location of the malformation.[4] More detailed pictures of the tangle of blood vessels that compose an AVM can be obtained by using radioactive agents injected into the blood stream. If a CT is used in conjunction of dye this is called a computerized tomography angiogram while if MRI is used it is called magnetic resonance angiogram.[1][4] The best images of an AVM are obtained through cerebral angiography. This procedure involves using a catheter, threaded through an artery up to the head, to deliver a contrast agent into the AVM. As the contrast agent flows through the AVM structure, a sequence of X-ray images are obtained.[4]
Grading
A common method of grading cerebral AVMs is the Spetzler-Martin grade.[5] This system was designed to assess the patient's risk of neurological deficit after open surgical resection, based on characteristics of the AVM itself. Based on this system, AVMs may be classified as grades 1 - 5.
AVM size Adjacent eloquent cortex Draining veins Under 3 cm = 1 Non-eloquent = 0 Superficial only = 0 3-6 cm = 2 Eloquent* = 1 Deep veins = 1 Over 6 cm = 3 - Such as sensory or motor cortex, language or visual areas, brain stem, etc.
The risk of post-surgical neurological deficit (difficulty with language, motor weakness, vision loss) increases with increasing Spetzler-Martin grade.
Pathophysiology
AVMs are an abnormal connection between the arteries and veins in the human brain. Arteriovenous malformations are most commonly of prenatal origin.[6] The cause of AVMs remains unknown.[6] In a normal brain oxygen enriched blood from the heart travels in sequence through smaller blood vessels going from arteries, to arterioles and then capillaries.[6] Oxygen is removed in the latter vessel to be used by the brain.[6] After the oxygen is removed blood reaches venules and later veins which will take it back to the heart and lungs.[6] On the other hand when there is an AVM blood goes directly from arteries to veins through the abnormal vessels disrupting the normal circulation of blood.[6]
Prognosis
The main risk is intracranial hemorrhage. This risk is difficult to quantify since many patients with asymptomatic AVMs will never come to medical attention. Small AVMs tend to bleed more often than do larger ones, the opposite of cerebral aneurysms.[7] If a rupture or bleeding incident occurs, the blood may penetrate either into the brain tissue (cerebral hemorrhage) or into the subarachnoid space, which is located between the sheaths (meninges) surrounding the brain (subarachnoid hemorrhage). Bleeding may also extend into the ventricular system (intraventricular hemorrhage). Cerebral hemorrhage appears to be most common. [1] One long-term study (mean follow up greater than 20 years) of over 150 symptomatic AVMs (either presenting with bleeding or seizures) found the risk of cerebral hemorrhage to be approximately 4% per year, slightly higher than the 2-3% seen in other studies.[8] A simple, rough approximation of a patient's lifetime bleeding risk is 105 - (patient age in years).[9] This equation assumes a 3% yearly bleeding risk. For example, a healthy 30 year old patient would have approximately a 75% lifetime risk of at least one bleeding event.
Treatment
Treatment depends on the location and size of the AVM and whether there is bleeding or not.[10]
The treatment in the case of sudden bleeding is focused on restoration of vital function. Anticonvulsant medications such as phenytoin are often used to control seizure; medications or procedures may be employed to relieve intracranial pressure. Eventually, curative treatment may be required to prevent recurrent hemorrhage. However, any type of intervention may also carry a risk of creating a neurological deficit.[citation needed]
Surgical elimination of the blood vessels involved is the preferred curative treatment for many types of AVM.[10] Surgery is performed by a neurosurgeon who temporarily removes part of the skull (craniotomy), separates the AVM from surrounding brain tissue, and resects the abnormal vessels.[10] While surgery can result in an immediate, complete removal of the AVM, risks exist depending on the size and the location of the malformation. The preferred treatment of Spetzler-Martin grade 1 and 2 AVMs in young, healthy patients is surgical resection due to the relatively small risk of neurological damage compared to the high lifetime risk of hemorrhage. Grade 3 AVMs may or may not be amenable to surgery. Grade 4 and 5 AVMs are not usually surgically treated.[11]
Radiosurgery has been widely used on small AVMs with considerable success. The Gamma Knife is an apparatus used to precisely apply a controlled radiation dosage to the volume of the brain occupied by the AVM. While this treatment does not require an incision and craniotomy (with their own inherent risks), three or more years may pass before the complete effects are known, during which time patients are at risk of bleeding.[10] Complete obliteration of the AVM may or may not occur after several years, and repeat treatment may be needed. Radiosurgery is itself not without risk. In one large study, nine percent of patients had transient neurological symptoms, including headache, after radiosurgery for AVM. However, most symptoms resolved, and the long-term rate of neurological symptoms was 3.8%.[12]
Embolization is the occlusion of blood vessels most commonly with a glue-like substance introduced by a radiographically guided catheter.[10] Such glue blocks the vessel and reduces blood flow into the AVM.[10] Embolization is frequently used as an adjunct to either surgery or radiation treatment.[10] Before other treatments it reduces the size of the AVM while during surgery it reduces the risk of bleeding.[10] However, embolization alone may completely obliterate some AVMs.
Epidemiology
The annual new detection rate incidence of AVMs is approximately 1 per 100000 a year. The point prevalence in adults is approximately 18 per 100000.[1] AVMs are more common in males than females, although in females pregnancy may start or worsen symptoms due the increase in blood flow and volume it usually brings.[13]
Research directions
No randomized, controlled clinical trial has established a survival benefit for treating patients (either with open surgery or radiosurgery) with AVMs that have not yet bled. An international study is currently under way to evaluate the best management strategy for patients with unruptured AVMs.[14]
References
- ^ a b c d e Al-Shahi R, Warlow C (October 2001). "A systematic review of the frequency and prognosis of arteriovenous malformations of the brain in adults". Brain 124 (Pt 10): 1900–26. doi:10.1093/brain/124.10.1900. PMID 11571210. http://brain.oxfordjournals.org/cgi/content/full/124/10/1900?view=long&pmid=11571210. Retrieved 2010-05-18.
- ^ a b c Mayo Clinic staff (02 2009). "Brain AVM (arteriovenous malformation)-Symptoms". Mayo Foundation for Medical Education and Research. http://www.mayoclinic.com/health/brain-avm/DS01126/DSECTION=symptoms. Retrieved 2010-05-18.
- ^ a b c d David C. Dugdale, Daniel B. Hoch (10 2008). "Arteriovenous malformation - cerebral". ADAM. http://www.nlm.nih.gov/medlineplus/ency/article/000779.htm. Retrieved 2010-05-18.
- ^ a b c d e Mayo Clinic staff (02 2009). "Brain AVM (arteriovenous malformation)-Tests and diagnosis". Mayo Foundation for Medical Education and Research. http://www.mayoclinic.com/health/brain-avm/DS01126/DSECTION=tests-and-diagnosis. Retrieved 2010-05-18.
- ^ Spetzler, R; Martin N (1986). "A proposed grading system for arteriovenous malformations". J Neurosurg 65 (4): 476–83. doi:10.3171/jns.1986.65.4.0476. PMID 3760956.
- ^ a b c d e f Mayo Clinic staff (02 2009). "Brain AVM (arteriovenous malformation)-Causes". Mayo Foundation for Medical Education and Research. http://www.mayoclinic.com/health/brain-avm/DS01126/DSECTION=causes. Retrieved 2010-05-30.
- ^ Crawford, PM; et al (1986). "Arteriovenous malformations of the brain: natural history in unoperated patients". J Neurol Neurosurg Psychiatry 49 (1): 1–10. doi:10.1136/jnnp.49.1.1. PMC 1028639. PMID 3958721. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1028639.
- ^ Ondra, SL; et al (1990). "The natural history of symptomatic arteriovenous malformations of the brain: A 24-year follow-up assessment". J Neurosurgery 73 (3): 387–391. doi:10.3171/jns.1990.73.3.0387. PMID 2384776.
- ^ Greenberg, Mark (2010). Handbook of Neurosurgery (7th ed). Thieme. pp. 1100.
- ^ a b c d e f g h Mayo Clinic staff (02 2009). "Brain AVM (arteriovenous malformation)-Treatments and drugs". Mayo Foundation for Medical Education and Research. http://www.mayoclinic.com/health/brain-avm/DS01126/DSECTION=treatments-and-drugs. Retrieved 2010-05-18.
- ^ Starke, RM; et al (2009). "Treatment guidelines for cerebral arteriovenous malformation microsurgery". Br J Neurosurg 23 (4): 376–86. doi:10.1080/02688690802562663. PMID 19637008.
- ^ Flickinger, JC; et al (1998). "Analysis of neurological sequelae from radiosurgery of arteriovenous malformations: How location affects outcome". Int J Radiat Oncol Biol Phys 40 (2): 273–278. doi:10.1016/S0360-3016(97)00718-9. PMID 9457809.
- ^ Mayo Clinic staff (02 2009). "Brain AVM (arteriovenous malformation)-Risk factors". Mayo Foundation for Medical Education and Research. http://www.mayoclinic.com/health/brain-avm/DS01126/DSECTION=risk-factors. Retrieved 2010-05-30.
- ^ "The ARUBA trial-A Randomized Trial of Unruptured Brain Arteriovenous Malformations". http://arubastudy.org/. Retrieved 2010-05-30.
External links
Congenital vascular defects / Vascular malformation (Q25–Q28, 747) Great arteries/
other arteriesPulmonary atresia · Stenosis of pulmonary arterySingle umbilical arteryGreat veins Arteriovenous malformation Cerebral arteriovenous malformationCategories:- Anatomical pathology
- Congenital vascular defects

Wikimedia Foundation. 2010.