- Scoliosis
-
Scoliosis Classification and external resources 
ICD-10 M41 ICD-9 737.3,737.43,754.2 Scoliosis (from Greek: skoliōsis meaning from skolios, "crooked")[1] is a medical condition in which a person's spine is curved from side to side. Although it is a complex three-dimensional deformity, on an X-ray, viewed from the rear, the spine of an individual with scoliosis may look more like an "S" or a "C" than a straight line. Scoliosis is typically classified as either congenital (caused by vertebral anomalies present at birth), idiopathic (cause unknown, subclassified as infantile, juvenile, adolescent, or adult, according to when onset occurred), or neuromuscular (having developed as a secondary symptom of another condition, such as spina bifida, cerebral palsy, spinal muscular atrophy, or physical trauma).
Contents
Signs and symptoms
Patients having reached skeletal maturity are less likely to have a worsening case. Some severe cases of scoliosis can lead to diminishing lung capacity, putting pressure on the heart, and restricting physical activities.
The signs of scoliosis can include:
- Uneven musculature on one side of the spine
- A rib prominence and/or a prominent shoulder blade, caused by rotation of the ribcage in thoracic scoliosis
- Uneven hips/leg lengths
- Slow nerve action (in some cases)
Associated conditions
Scoliosis is sometimes associated with other conditions such as Ehlers–Danlos syndrome (hyperflexibility, "floppy baby" syndrome, and other variants of the condition), Charcot–Marie–Tooth disease, Prader–Willi syndrome, kyphosis, cerebral palsy, spinal muscular atrophy, muscular dystrophy, familial dysautonomia, CHARGE syndrome, Friedreich's ataxia, Fragile X syndrome[2][3], proteus syndrome, spina bifida, Marfan's syndrome, neurofibromatosis, connective tissue disorders, congenital diaphragmatic hernia, hemihypertrophy, and craniospinal axis disorders (e.g., syringomyelia, mitral valve prolapse, Arnold–Chiari malformation), and Amniotic Band Syndrome (ABS).
Scoliosis associated with known syndromes such as Marfan's or Prader–Willi is often sub-classified as "syndromic scoliosis."
Cause
It has been estimated that approximately 65% of scoliosis cases are idiopathic, approximately 15% are congenital and approximately 10% are secondary to a neuromuscular disease.[4]
Idiopathic scoliosis is a condition which lasts a lifetime, but it does not increase the risk of mortality.[5]
In adolescent idiopathic scoliosis, there is no clear causal agent and it is generally believed to be multifactorial, although genetics are believed to play a role.[6] Various causes have been implicated, but none of them have consensus among scientists as the cause of scoliosis, though the role of genetic factors in the development of this condition is widely accepted.[7] Still, at least one gene, notably CHD7, has been associated with the idiopathic form of scoliosis.[8][7]
In some cases, scoliosis exists at birth due to a congenital vertebral anomaly.
Scoliosis secondary to neuromuscular disease may develop during adolescence, such as with tethered spinal cord syndrome.[9] Scoliosis often presents itself, or worsens, during the adolescence growth spurt and is more often diagnosed in females versus males.
Diagnosis
 Cobb angle measurement of a levoscoliosis
Cobb angle measurement of a levoscoliosis
Patients who initially present with scoliosis are examined to determine whether there is an underlying cause of the deformity. During a physical examination, the following is assessed:
- Skin for café au lait spots, indicative of neurofibromatosis
- The feet for cavovarus deformity
- Abdominal reflexes
- Muscle tone for spasticity
During the exam, the patient is asked to remove his or her shirt and bend forward. This is known as the Adams Forward Bend Test[10] and is often performed on school students. If a prominence is noted, then scoliosis is a possibility and the patient should be sent for an X-ray to confirm the diagnosis.
As an alternative, a scoliometer may be used to diagnose the condition.[11] The patient's gait is assessed, and there is an exam for signs of other abnormalities (e.g., spina bifida as evidenced by a dimple, hairy patch, lipoma, or hemangioma). A thorough neurological examination is also performed.
It is usual, when scoliosis is suspected, to arrange for weight-bearing full-spine AP/coronal (front-back view) and lateral/sagittal (side view) X-rays to be taken. This is to assess the scoliosis curves and the kyphosis and lordosis, as these can also be affected in individuals with scoliosis. Full-length standing spine X-rays are the standard method for evaluating the severity and progression of the scoliosis, and whether it is congenital or idiopathic in nature. In growing individuals, serial radiographs are obtained at 3–12 month intervals to follow curve progression, and, in some instances, MRI investigation is warranted to look at the spinal cord.
The standard method for assessing the curvature quantitatively is measurement of the Cobb angle, which is the angle between two lines, drawn perpendicular to the upper endplate of the uppermost vertebrae involved and the lower endplate of the lowest vertebrae involved. For patients with two curves, Cobb angles are followed for both curves. In some patients, lateral-bending X-rays are obtained to assess the flexibility of the curves or the primary and compensatory curves.
Genetic testing
Genetic testing for AIS, which became available in 2009 and is still under investigation, attempts to gauge the likelihood of curve progression.
Through a genome-wide association study, geneticists have identified single nucleotide polymorphism markers in the DNA that are significantly associated with adolescent idiopathic scoliosis. Fifty-three genetic markers have been identified. Scoliosis has been described as a biomechanical deformity, the progression of which is dependent on asymmetric forces otherwise known as the Heuter-Volkmann law.[12][13]
Management
The traditional medical management of scoliosis is complex and is determined by the severity of the curvature and skeletal maturity, which together help predict the likelihood of progression.
The conventional options are, in order:
- Observation
- Physical Therapy
- Occupational Therapy
- Chiropractic or Osteopathic Therapy
- Casting (EDF)
- Bracing
- Surgery
A growing body of scientific research testifies to the efficacy of specialized treatment programs of physical therapy, which may include bracing.[14] Debate in the scientific community about whether chiropractic and physical therapy can influence scoliotic curvature is partly complicated by the variety of methods proposed and employed: Some are supported by more research than others.[15][not in citation given]
Physiotherapy
The Schroth method is a noninvasive, physiotherapeutic treatment, which has been used successfully in Europe since the 1920s.[16][17] Originally developed in Germany by scoliosis sufferer Katharina Schroth, this method is now taught to scoliosis patients in clinics specifically devoted to Schroth therapy in Germany, Spain, England, and North America. The method is based upon the concept of scoliosis as resulting from a complex of muscular asymmetries (especially strength imbalances in the back) that can be at least partially corrected by targeted exercises.[17]
The Schroth method has proven effective at reversing abnormal scoliotic curvatures by an average of 10% in 4- to 6-week in-patient programs,[18] and by 30% or more in an out-patient program over a period of a year.[19] One study of nearly 200 adolescent Schroth patients found no curve progression three years following the in-patient program.[20] Several studies have documented the Schroth method's efficacy in substantially reducing or eliminating pain, which tends to be a problem, in particular, for adults.[21]
Small curvatures between 15 and 20° during growth may be treated with the physio-logic-program,[22] curvatures between 20 and 30° during growth spurt with "3D-made-easy". This program has been tested in the environment of in-patient treatment as well.[23][24] In curvatures exceeding 30°, a combination of the methods described together with the Schroth program may be helpful,[25] and a specialized centre with trained and certified staff should be taken into account. Out-patient rehabilitation treatments today may reach the same outcome as in-patient programs.[26] Out-patient programs may be successful when pattern-specific programs are provided. A certain intensity is necessary to allow the very best compliance with conservative treatment, and to acquire strategies for coping with scoliosis and with the conservative treatment.
The indications for treatment depend on degree of curvature, maturity of the patient, and the individual curve pattern. While evidence supporting such conservative, non-invasive treatments is weak, today conservative management of scoliosis can be regarded as being evidence-based; no substantial evidence has been found to support surgical intervention.[27]
Occupational Therapy
An occupational therapist (OT) helps those having experienced an injury or illness regain or maintain the ability to participate in their everyday activities. For those with scoliosis, an occupational therapist can provide assistance through assessment, intervention, and ongoing evaluation of the condition, which will help them manage physical symptoms so they can participate in daily activities, such as those in self-care, productivity, and leisure.
One intervention involves bracing. During the past several decades, a large variety of bracing devices have been developed for the treatment of scoliosis.[28] Studies demonstrate that presenting force sideways across a joint by bracing prevents further curvature of the spine in idiopathic scoliosis,[29] while other studies have also shown that braces can be used by individuals with scoliosis during physical activities.[30]
Other interventions include postural strategies such as posture training in sitting, standing, and sleeping positions and in using positioning supports such as pillows, wedges, rolls, and corsets.[31]
Adaptive and compensatory strategies are also employed to help facilitate individuals to returning daily activities.
Self-care
Disability caused by scoliosis, as well as physical limitations during recovery from treatment related surgery, often affects an individual’s ability to perform self-care activities.[32] One of the first treatments of scoliosis is the attempt to prevent further curvature of the spine. Depending on the size of the curvature, this is typically done in one of three ways: bracing, surgery, or postural positioning through customized cushioning.[32][33][34] Stopping the progression of the scoliosis can prevent the loss of function in many activities of daily living by maintaining range of motion, preventing deformity of the rib cage, and reducing pain during activities such as bending or lifting.
Occupational therapists are often involved in the process of selection and fabrication of customized cushions. These individualized postural supports are used to maintain the current spinal curvature, or they can be adjusted to assist in the correction of the curvature. This type of treatment can help to maintain mobility for a wheelchair user by preventing the deformity of the rib cage and maintaining an active range of motion in the arms.[32]
For other self-care activities (such as dressing, bathing, grooming, personal hygiene, and feeding), several strategies can be used as a part of occupational therapy treatment. Environmental adaptations for bathing could include a bath bench, grab bars installed in the shower area, or a handheld shower nozzle.[35] For activities such as dressing and grooming, various assistive devices and strategies can be used to promote independence. An occupational therapist may recommend a long-handled reacher that can be used to assist independent dressing by allowing a person to avoid painful movements such as bending over; a long-handled shoehorn can be used for putting on and removing shoes. Problems with activities such as cutting meat and eating can be addressed by using specialized cutlery, kitchen utensils, or dishes.
Productivity
Productive activities include paid or unpaid work, household chores, school, work, and play.[36] Recent studies in healthcare have led to the development of a variety of treatments to assist in the management of scoliosis thereby maximizing productivity for people of all ages. Assistive technology has undergone dramatic changes over the past 20 years; the availability and quality of the technology has improved greatly.[37] As a result of using assistive technology, functional changes may range from improvements in abilities, performance in daily activities, participation levels, and quality of life.[36]
A common assistive technology intervention is specialized seating and postural control. It is widely known that, for children with poor postural control, a comfortable seating system that provides them with the support needed to maintain a sitting position can be essential for raising their overall level of well-being.[38] A child's well-being in a productive sense involves the ability to participate in classroom and play activities.[36] Specialized wheelchair seating has been identified as the most common prescription in the management of scoliosis in teenagers with muscular dystrophy.[39]
With comfortable wheelchair seating, teenagers are able to participate in classroom activities for longer periods with less fatigue. By tilting the seating position 20 degrees forward (toward the thighs), seating pressure is significantly redistributed, and, therefore, sitting is more comfortable. If an office worker with scoliosis can sit for longer periods, increased work output is likely to occur and could improve quality of life. Tall, forward sloping seats or front parts of seats, and when possible with tall desk with the opposite slope, can, in general, reduce pains and the need of bending significantly while working or studying, and that is particularly important with braced, fragile, or tender backs. And open hip angle can benefit the used lung volume and respiration. [40][41]
For those not using a wheelchair, bracing may be used to treat scoliosis. Lifestyle changes are made to compensate for the proper use of spine braces.
Leisure
There are many physical symptoms that can prevent a person from engaging in physical leisurely activities, such as chest pains, back pains, shortness of breath, and limited spinal movement. The OT's role is to help individuals with scoliosis manage these physical symptoms so they can participate in physical leisure activities.
Bracing is a common strategy recommended by an OT, in particular, for individuals engaging in sports and exercise.[30] An OT is responsible for educating an individual on the advantages and disadvantages of different braces, proper ways to wear the brace, and the day-to-day care of the brace.
To help a person manage heart and lung symptoms such as shortness of breath or chest pains, an occupational therapist can teach the individual energy conservation techniques.[35] This includes scheduling routine breaks during the activity, as suitable for the individual. For example, an occupational therapist can recommend that a swimmer take breaks between laps to conserve energy. Other energy conservation strategies knowing the benefits of scheduled rest and efficient breathing techniques.[35] Adapting or modifying the exercise or sport is another way a person with scoliosis can do it.[35] Adapting the activity may change the difficulty of the sport or exercise. For example, it might mean taking breaks throughout an exercise. If a person with scoliosis is unable to participate in a sport or exercise, an OT can help the individual explore other physical activities that are suitable to his/her interests and capabilities. An OT and the person with scoliosis can explore enjoyable and meaningful participation in the sport/exercise in another capacity, such as coaching or refereeing.
Bracing
Bracing is normally done when the patient has bone growth remaining and is, in general, implemented to hold the curve and prevent it from progressing to the point where surgery is recommended. Braces are sometimes prescribed for adults to relieve pain related to scoliosis. Bracing involves fitting the patient with a device that covers the torso; in some cases, it extends to the neck. The most commonly used brace is a TLSO, a corset-like appliance that fits from armpits to hips and is custom-made from fiberglass or plastic. It is sometimes worn 22–23 hours a day, depending on the doctor's prescription, and applies pressure on the curves in the spine. The effectiveness of the brace depends not only on brace design and orthotist skill but on patient compliance and amount of wear per day. The typical use of braces is for idiopathic curves that are not grave enough to warrant surgery, but they may also be used to prevent the progression of more severe curves in young children, to buy the child time to grow before performing surgery, which would prevent further growth in the part of the spine affected.
Bracing may cause emotional and physical discomfort. Physical activity may become more difficult because the brace presses against the stomach, making it difficult to breathe. Children may lose weight from the brace, due to increased pressure on the abdominal area.
The Scoliosis Research Society's recommendations for bracing include curves progressing to larger than 25 degrees, curves presenting between 30 and 45 degrees, Risser Sign 0, 1, or 2 (an X-ray measurement of a pelvic growth area), and less than 6 months from the onset of menses in girls.[42]
Progressive scolioses exceeding 25° Cobb in the pubertal growth spurt should be treated with a pattern-specific brace like the Chêneau brace and its derivates with an average brace-wearing time of 16 hours/day (23 hours/day assures the best possible result).
The latest standard of brace construction is with CAD/CAM technology. With the help of this technology it has been possible to standardize the pattern-specific brace treatment. Severe mistakes in brace construction are largely ruled out with the help of these systems. This technology also eliminates the need to make a plaster cast for brace construction. The measurements can be taken any place and is simple (and not comparable to plastering). In Germany, available CAD/CAM braces are known such as the Regnier-Chêneau brace, the Rigo-System-Chêneau-brace (RSC brace), and the Gensingen Brace, according to Weiss.[43] Many patients prefer the "Chêneau light" brace: It has the best in-brace corrections reported in international literature and is easier to wear than other braces in use today.[44][45] However, this brace is not available for all curve patterns.
In infantile and sometimes juvenile scoliosis, a plaster jacket applied early may be used instead of a brace. It has been proven possible[46] to permanently correct cases of infantile idiopathic scoliosis by applying a series of plaster casts (EDF: elongation, derotation, flexion) on a specialized frame under corrective traction, which helps to "mould" the infant's soft bones and work with their growth spurts. This method was pioneered by UK scoliosis specialist Min Mehta. Today, however, CAD/CAM braces are available for young children with a certain standard. Therefore, plaster jackets are now generally regarded as outdated.[43]
Surgery

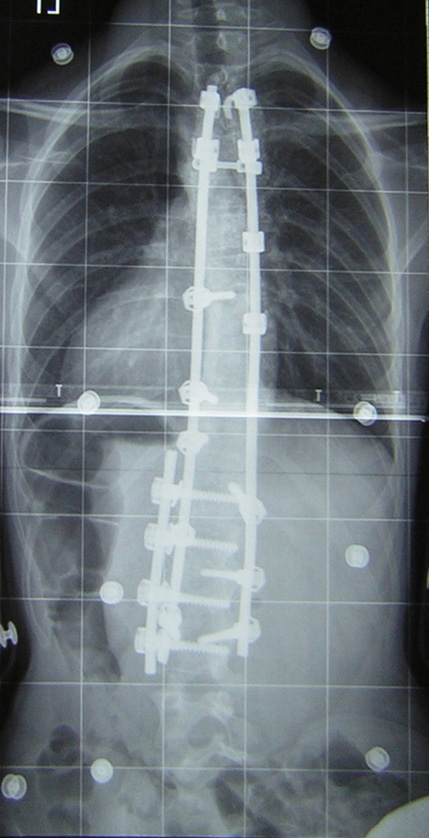
 Pre op (left) and post op (right) X-ray of a person with thoracic dextroscoliosis and lumbar levoscoliosis. The X-ray is usually projected such that the right side of the subject is on the right side of the image; i.e., the subject is viewed from the rear (see left image; the right image is seen from the front). This projection is typically used by surgeons, as it is how surgeons see their patients when they are on the operating table. Surgery was a fusion and instrumentation.
Pre op (left) and post op (right) X-ray of a person with thoracic dextroscoliosis and lumbar levoscoliosis. The X-ray is usually projected such that the right side of the subject is on the right side of the image; i.e., the subject is viewed from the rear (see left image; the right image is seen from the front). This projection is typically used by surgeons, as it is how surgeons see their patients when they are on the operating table. Surgery was a fusion and instrumentation.Surgery is usually recommended by orthopedists for curves that have a high likelihood of progression (i.e., greater than 45 to 50 degrees magnitude), curves that would be cosmetically unacceptable as an adult, curves in patients with spina bifida and cerebral palsy that interfere with sitting and care, and curves that affect physiological functions such as breathing.
Surgery for scoliosis is performed by a surgeon specializing in spine surgery. For various reasons, it is usually impossible to completely straighten a scoliotic spine, but in most cases significant corrections are achieved.
There are two main types of surgery:
- Anterior fusion: This surgical approach is through an incision (cut) at the side of the chest wall
- Posterior fusion: This surgical approach is through an incision on the back and involves the use of metal instrumentation to correct the curve.
One or both of these surgical procedures may be needed. The surgery may be done in one or two stages and, on average, will take four to eight hours.
Spinal fusion with instrumentation
Spinal fusion is the most widely performed surgery for scoliosis. In this procedure, bone (either harvested from elsewhere in the body autograft or from a donor allograft) is grafted to the vertebrae so that when it heals they will form one solid bone mass and the vertebral column becomes rigid. This prevents worsening of the curve, at the expense of some spinal movement. This can be performed from the anterior (front) aspect of the spine by entering the thoracic or abdominal cavity or, more commonly, performed from the back (posterior). A combination is used in more severe cases.
Spinal fusions were once performed without metal implants.[citation needed] In this technique, a cast was applied after the surgery, usually under traction to pull the curve as straight as possible and then hold it there while fusion took place. Casting left patients largely immobilized for a period of weeks to months, with significant burden on patient quality of life. Additionally, there was a relatively high risk of pseudarthrosis (fusion failure) at one or more levels, and significant correction could not always be achieved.
In 1962, Paul Harrington introduced a metal spinal system of instrumentation that assisted with straightening the spine, as well as holding it rigid while fusion took place. The original (now obsolete) Harrington rod operated on a ratchet system, attached by hooks to the spine at the top and bottom of the curvature that when cranked would distract, or straighten, the curve. The Harrington rod represented a major advance in the field, as it obviated the need for prolonged casting, allowing patients greater mobility in the post-operative period and significantly reducing the quality of life burden of fusion surgery. Additionally, as the first system to apply instrumentation directly to the spine, the Harrington rod was the precursor to most modern spinal instrumentation systems. A major shortcoming of the Harrington method was that it failed to produce a posture wherein the skull would be in proper alignment with the pelvis, and it did not address rotational deformity. As a result, unfused parts of the spine would try to compensate for this in the effort to stand up straight. As the person aged, there would be increased wear and tear, early-onset arthritis, disc degeneration, muscular stiffness, and pain with eventual reliance on painkillers, further surgery, inability to work full-time, and disability. "Flatback" became the medical name for a related complication, especially for those who had lumbar scoliosis.[47]
Modern spinal systems are attempting to address sagittal imbalance and rotational defects unresolved by the Harrington rod system. They involve a combination of rods, screws, hooks, and wires fixing the spine, and can apply stronger, safer forces to the spine than the Harrington rod. This technique is known as the Cotrel-Dubousset instrumentation, currently the most common technique for the procedure.
In general, modern spinal fusions have good outcomes with high degrees of correction and low rates of failure and infection. Patients with fused spines and permanent implants tend to have normal lives with unrestricted activities when they are younger; it remains to be seen whether those that have been treated with the newer surgical techniques develop problems as they age.[48]
Pedicle screw-only posterior spinal fusion may improve major curve correction at 2 years among patients with adolescent idiopathic scoliosis (AIS) as compared to hybrid instrumentation (proximal hooks with distal pedicle screws) (65% versus 46%) according to a retrospective matched cohort study.[49] The prospective cohorts were matched to the retrospective cohorts according to patient age, fusion levels, Lenke curve type, and operative method. The two groups were not significantly different in regard to age, Lenke AIS curve type, or Riser grade. The numbers of fused vertebrae were significantly different (11.7±1.6 for pedicle screw versus 13.0±1.2 for hybrid group). This study's results may be biased due to the pedicle screw group's being analyzed prospectively versus retrospective analysis of the hybrid instrumentation group.
Thoracoplasty
A complementary surgical procedure a surgeon may recommend is called thoracoplasty (also called costoplasty). This is a procedure to reduce the rib hump that affects most scoliosis patients with a thoracic curve. A rib hump is evidence that there is some rotational deformity to the spine. Thoracoplasty may also be performed to obtain bone grafts from the ribs instead of the pelvis, regardless of whether a rib hump is present. Thoracoplasty can be performed as part of a spinal fusion or as a separate surgery, entirely.
Thoracoplasty is the removal (or resection) of typically four to six segments of adjacent ribs that protrude. Each segment is one to two inches long. The surgeon decides which ribs to resect based on either their prominence or their likelihood to be realigned by correction of the curvature alone. The ribs grow back, and will grow back straight.
Thoracoplasty has risks, such as increased pain in the rib area during recovery or reduced pulmonary function (10–15 percent is typical) following surgery. This impairment can last anywhere from a few months to two years. Because thoracoplasty may lengthen the duration of surgery, patients may also lose more blood or develop complications from the prolonged anesthesia. A more significant, though far less common, risk is that the surgeon will inadvertently puncture the pleura, a protective coating over the lungs. This could cause blood or air to drain into the chest cavity, conditions called a haemothorax or pneumothorax, respectively.[50]
Complications
The risk of undergoing surgery for scoliosis is estimated to be 5%. Possible complications may be inflammation of the soft tissue or deep inflammatory processes, breathing impairments, bleeding and nerve injuries. However, according to the latest evidence, the rate of complications is far higher. As early as five years after surgery another 5% require reoperation and today it is not yet clear what to expect from spine surgery in the long-term.[51][52] Taking into account that signs and symptoms of spinal deformity cannot be changed by surgical intervention, surgery remains primarily a cosmetic indication[dubious ], only especially in patients with adolescent idiopathic scoliosis (AIS), the most common form of scoliosis never exceeding 80°.[51][53] However, the cosmetic effects of surgery are not necessarily stable.[51]
In case one decides to undergo surgery, a specialized center should be preferred.
Surgery without fusion
New implants that aim to delay spinal fusion and to allow more spinal growth in young children have been developed. For the youngest patients, whose thoracic insufficiency compromises their ability to breathe and applies significant cardiac pressure, ribcage implants that push the ribs apart on the concave side of the curve may be especially useful. These vertical expandable prosthetic titanium ribs (VEPTR) provide the benefit of expanding the thoracic cavity and straightening the spine in all three dimensions while allowing it to grow.
Although these methods are novel and promising, these treatments are suitable only for growing patients. Spinal fusion remains the "gold standard" of surgical treatment for scoliosis.[47]
Prognosis
The prognosis of scoliosis depends on the likelihood of progression. The general rules of progression are that larger curves carry a higher risk of progression than smaller curves, and that thoracic and double primary curves carry a higher risk of progression than single lumbar or thoracolumbar curves. In addition, patients not having yet reached skeletal maturity have a higher likelihood of progression (i.e., if the patient has not yet completed the adolescent growth spurt). Females have a greater risk of progression as well.[citation needed]
Epidemiology
This condition affects approximately 7 million people in the United States.[54] A scoliosis spinal columns curve of 10° or less affects 1.5% to 3% of individuals.[42] The prevalence of curves less than 20° is about equal in males and females. It is most common during late childhood, in particular, in girls.[55]
Society and culture
Scoliosis Research Society
Main article: Scoliosis Research SocietyThe Scoliosis Research Society is a professional organization of physicians and allied health personnel. Their primary focus is on providing continuing medical education for healthcare professionals and on funding/supporting research in spinal deformities. Founded in 1966, the SRS has gained recognition as one of the world's premier spine societies. Strict membership criteria ensure that the individual Fellows support that commitment. Current membership includes over 1,000 of the world's leading spine surgeons as well as some researchers, physician assistants, and orthotists who are involved in research and treatment of spinal deformities. The purpose of the Scoliosis Research Society is to foster the optimal care of all patients with spinal deformities.[56]
About Skolyoz Destek Grubu
Skolyoz Destek Grubu is a non-profit network organization of Scoliosis patient groups, provides information on the diagnosis, treatment and care of persons living with scoliosis and supports its member organisations in the fulfilment of their missions.
Skolyoz Destek Grubu also advocates, both independently and in collaboration with organisations with similar objectives.
See also
- Kyphosis
- Hyperkyphosis
- Lordosis
- Pott's disease
- Scheuermann's disease
- Schooliosis
- Neuromechanics of idiopathic scoliosis
- Back brace
References
- ^ Online Etymology Dictionary. Douglas Harper, Historian. Accessed 27 December 2008. Dictionary.com
- ^ "Fragile X syndrome". Department for Work and Pensions, U.K.. http://www.dwp.gov.uk/publications/specialist-guides/medical-conditions/a-z-of-medical-conditions/learning-disability/fragile-x-syndrome-ld.shtml. Retrieved 29 August 2011.
- ^ "Orthopaedic aspects of fragile-X syndrome". The National Center for Biotechnology Information. http://www.ncbi.nlm.nih.gov/pubmed/2195034. Retrieved 29 August 2011.
- ^ Page 90 in: Elizabeth D Agabegi; Agabegi, Steven S. (2008). Step-Up to Medicine (Step-Up Series). Hagerstwon, MD: Lippincott Williams & Wilkins. ISBN 0-7817-7153-6.
- ^ Asher, Marc A.. "Adolescent idiopathic scoliosis: natural history and long term treatment effects". BioMed central. http://www.biomedcentral.com/content/pdf/1748-7161-1-2.pdf. Retrieved 7 November 2011.
- ^ Kouwenhoven JW, Castelein RM (2008). "The pathogenesis of adolescent idiopathic scoliosis: review of the literature". Spine 33 (26): 2898–2908. doi:10.1097/BRS.0b013e3181891751. PMID 19092622.
- ^ a b Ogilvie JW, Braun J, Argyle V, Nelson L, Meade M, Ward K (2006). "The search for idiopathic scoliosis genes". Spine 31 (6): 679–681. doi:10.1097/01.brs.0000202527.25356.90. PMID 16540873.
- ^ Texas Scottish Rite Hospital for Children
- ^ "Scoliosis — Causes — Risk Factors". PediatricHealthChannel. http://www.pediatrichealthchannel.com/scoliosis/causes.shtml.
- ^ "Scoliosis symptoms — pain, flat back, screening, self-assessment". iscoliosis.com. http://www.iscoliosis.com/symptoms.html.
- ^ "Scoliometer (Inclinometer)". National Scoliosis Foundation. http://www.scoliosis.org/store/scoliometer.php.
- ^ US patent 6,773,437, Ogilvie J, Drewry TD, Sherman MC, Saurat J, "Shape memory alloy staple", issued 2004-08-10
- ^ Ogilvie J (2010). "Adolescent idiopathic scoliosis and genetic testing". Current Opinion in Pediatrics 22 (1): 67–70. doi:10.1097/MOP.0b013e32833419ac. PMID 19949338.
- ^ Negrini S, Fusco C, Minozzi S, Atanasio S, Zaina F, Romano M (2008). "Exercises reduce the progression rate of adolescent idiopathic scoliosis: results of a comprehensive systematic review of the literature". Disability and Rehabilitation 30 (10): 772–785. doi:10.1080/09638280801889568. PMID 18432435.
- ^ Majdouline Y, Aubin CE, Robitaille M, Sarwark JF, Labelle H (2007). "Scoliosis correction objectives in adolescent idiopathic scoliosis". Journal of Pediatric Orthopedics 27 (7): 775–781. doi:10.1097/BPO.0b013e31815588d8. PMID 17878784.
- ^ Lehnert-Schroth C (2000). Dreidimensionale Skoliosebehandlung (6th ed.). Stuttgart: Urban & Schwarzer.[page needed]
- ^ a b Lehnert-Schroth C (2007). Three-Dimensional Treatment for Scoliosis: A Physiotherapeutic Method for Deformities of the Spine. Palo Alto CA: The Martindale Press. pp. 1–6. ISBN 0914959026.
- ^ Weiss, HR (1992). "Influence of an in-patient exercise program on scoliotic curve". Italian journal of orthopaedics and traumatology 18 (3): 395–406. PMID 1308886.
- ^ Otman, S; Kose, N; Yakut, Y (2005). "The efficacy of Schroth s 3-dimensional exercise therapy in the treatment of adolescent idiopathic scoliosis in Turkey". Saudi medical journal 26 (9): 1429–35. PMID 16155663.
- ^ Weiss, HR; Lohschmidt, K; El-Obeidi, N; Verres, C (1997). "Preliminary results and worst-case analysis of in patient scoliosis rehabilitation". Pediatric rehabilitation 1 (1): 35–40. PMID 9689236.
- ^ Weiss HR, "Scoliosis-related pain in adults: Treatment influences," European Journal of Physical Medicine and Rehabilitation 3/3 (1993): 91–94.
- ^ Weiss HR, Klein R (2006). "Improving excellence in scoliosis rehabilitation: a controlled study of matched pairs". Pediatric Rehabilitation 9 (3): 190–200. doi:10.1080/13638490500079583. PMID 17050397.
- ^ Weiss HR, Hollaender M, Klein R (2006). "ADL based scoliosis rehabilitation—the key to an improvement of time-efficiency?". Studies in Health Technology and Informatics 123: 594–8. PMID 17108494. http://booksonline.iospress.nl/Extern/EnterMedLine.aspx?ISSN=0926-9630&Volume=123&SPage=594.
- ^ Weiss HR, Maier-Hennes A (2008). "Specific exercises in the treatment of scoliosis—differential indication". Studies in Health Technology and Informatics 135: 173–90. PMID 18401090. http://booksonline.iospress.nl/Extern/EnterMedLine.aspx?ISSN=0926-9630&Volume=135&SPage=173.
- ^ Weiss HR (2010). Best Practice in Conservative Scoliosis Care (3rd ed.). Munich: Pflaum.[page needed]
- ^ Rigo M, Quera-Salvá G, Villagrasa M et al. (2008). "Scoliosis intensive out-patient rehabilitation based on Schroth method". Studies in Health Technology and Informatics 135: 208–27. PMID 18401092. http://booksonline.iospress.nl/Extern/EnterMedLine.aspx?ISSN=0926-9630&Volume=135&SPage=208.
- ^ Weiss HR, Goodall D (2008). "The treatment of adolescent idiopathic scoliosis (AIS) according to present evidence. A systematic review". European Journal of Physical and Rehabilitation Medicine 44 (2): 177–93. PMID 18418338. http://www.minervamedica.it/index2.t?show=R33Y2008N02A0177.
- ^ DeWald, RL (2003). Spinal Deformitities: The Comprehensive Text. New York: Thieme Medical Publishers, Inc.
- ^ Bulthuis G.J., Veldhuizen A.G., Nijenbanning G. (2008). "Clinical effect of continuous corrective force delivery in the non-operative treatment of idiopathic scoliosis: a prospective cohort study of the triac-brace". European Spine Journal 17 (2): 231–239. doi:10.1007/s00586-007-0513-9. PMC 2226193. PMID 17926071. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2226193.
- ^ a b Green BN, Johson C, Moreau C. (2009). "Is physical activity contraindicated for individuals with scoliosis? A systematic literature review". Journal of Chiropractic Medicine 8 (1): 25–37. doi:10.1016/j.jcm.2008.11.001. PMC 2697577. PMID 19646383. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2697577.
- ^ Paris MJ, Lang G, Benjamin MJ, Wilcox R. (2008). Standard of Care: Marfan Syndrome. Brigham and Womans Hospital. http://www.brighamandwomens.org/RehabilitationServices/Physical%20Therapy%20Standards%20of%20Care%20and%20Protocols/General%20-%20Marfan%20Syndrome.pdf.
- ^ a b c Burd TA, Pawelek L, Lenke LG. (2008). "Upper Extremity Functional Assessment After Anterior Spinal Fusion via Thoracotomy for Adolescent Idiopathic Scoliosis: Prospective Study of Twenty-Five Patients". Spine 27 (1): 65–71. doi:10.1097/00007632-200201010-00016. PMID 11805638.
- ^ Voda S. (2009). "Dangerous Curves: Treating adult idiopathic scoliosis". Nursing 39 (12): 42–6. doi:10.1097/01.NURSE.0000365025.40773.4c (inactive 2010-05-12). PMID 19934743.
- ^ Weiss H.F. (2003). "Rehabilitation of adolescent patients with scoliosis – What do we know? A review of the literature". Pediatric Rehabilitation 6 (3): 183–194.
- ^ a b c d Radomski, M.V. (2008). Occupational therapy for physical dysfunction sixth edition.. Philadelphia: Lippincott Williams & Wilkins. p. 964. ISBN 978-0-7817-6312-7. http://books.google.com/?id=hczaxaAXCDsC&pg=PA964.
- ^ a b c Rigby, P.J. (2009). Assistive technology for persons with physical disabilities: Evaluation and outcomes Thesis, Utrecht University, The Netherlands.. Toronto: University of Toronto Press. ISBN 978-90-393-50416.
- ^ Salter K, Jutai J, Teasell R, Foley NC, Bitensky J, Bayley M. (2010). "Issues for selection of outcome measures in stroke rehabilitation: ICF activity". Disability and Rehabilitation 27 (6): 315–340. doi:10.1080/09638280400008545. PMID 16040533.
- ^ Telfer S., Solomonidis S., Spence W. (2009). "An investigation of teaching staff members' and parents' views on the current state of adaptive seating technology and provision". Disability & Rehabilitation: Assistive Technology 5 (1): 14–24. doi:10.3109/17483100903191334. PMID 19941437.
- ^ Richardson M & Frank A.O. (2009). "Electric powered wheelchairs for those with muscular dystrophy: problems of posture, pain and deformity". Disability & Rehabilitation: Assistive Technology 4 (3): 181–188. doi:10.1080/17483100802543114.
- ^ Mandal A C 1996: Balanced Sitting Posture on Forward Sloping Seat
- ^ Mandal T 2009: Better furniture types for work and studies reduces bending and pain. Association for Body Conscious Design
- ^ a b Herring JA (2002). Tachdjian's Pediatric Orthopaedics. Philadelphia PA: W.B. Saunders. ISBN 0721656846.[page needed]
- ^ a b Weiss HR: Best Practice in conservative scoliosis care. Pflaum Company, 3rd. edition, Munich 2010[page needed]
- ^ Weiss HR, Werkmann M, Stephan C (2007). "Correction effects of the ScoliOlogiC® "Chêneau light" brace in patients with scoliosis". Scoliosis 2: 2. doi:10.1186/1748-7161-2-2. PMC 1805423. PMID 17257399. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1805423.
- ^ Weiss HR, Werkmann M, Stephan C (2007). "Brace related stress in scoliosis patients – Comparison of different concepts of bracing". Scoliosis 2: 10. doi:10.1186/1748-7161-2-10. PMC 2000861. PMID 17708766. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2000861.
- ^ Mehta MH (2005). "Growth as a corrective force in the early treatment of progressive infantile scoliosis". The Journal of Bone and Joint Surgery. British Volume 87 (9): 1237–1247. doi:10.1302/0301-620X.87B9.16124. PMID 16129750.
- ^ a b Scoliosis Surgery. News-medical.net. Retrieved on 2011-01-16.
- ^ Weill Cornell Neurological Surgery – Surgical Services. Cornellneurosurgery.org. Retrieved on 2011-01-16.
- ^ Kim YJ, Lenke LG, Kim J et al. (2006). "Comparative analysis of pedicle screw versus hybrid instrumentation in posterior spinal fusion of adolescent idiopathic scoliosis". Spine 31 (3): 291–298. doi:10.1097/01.brs.0000197865.20803.d4. PMID 16449901.
- ^ CurvedSpine.com Web site. Used with permission.
- ^ a b c Hawes M (2006). "Impact of spine surgery on signs and symptoms of spinal deformity". Pediatric Rehabilitation 9 (4): 318–39. PMID 17111548.
- ^ Weiss HR, Goodall D (2008). "Rate of complications in scoliosis surgery – a systematic review of the Pub Med literature". Scoliosis 3: 9. doi:10.1186/1748-7161-3-9. PMC 2525632. PMID 18681956. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=2525632.
- ^ Hawes MC, O'Brien JP (2008). "A century of spine surgery: what can patients expect?". Disability and Rehabilitation 30 (10): 808–817. doi:10.1080/09638280801889972. PMID 18432439.
- ^ Good, Christopher (2009). "The Genetic Basis of Adolescent Idiopathic Scoliosis". Journal of the spinal Research Foundation 4 (1): 13–5. http://www.spinemd.com/publications/articles/the-genetic-basis-of-adolescent-idiopathic-scoliosis.
- ^ Marieb, Elaine Nicpon (1998). Human anatomy & physiology. San Francisco: Benjamin Cummings. ISBN 0-8053-4360-1.[page needed]
- ^ Scoliosis Research Society website
Dorsopathies / spinal disease (M40–M54, 720–724, 737) Deforming dorsopathies OtherSpondylopathy inflammatory: Spondylitis (Ankylosing spondylitis) · Sacroiliitis · Discitis · Spondylodiscitis · Pott diseaseBack pain Intervertebral disc disorder M: JNT
anat(h/c, u, t, l)/phys
noco(arth/defr/back/soft)/cong, sysi/epon, injr
proc, drug(M01C, M4)
Congenital malformations and deformations of musculoskeletal system / musculoskeletal abnormality (Q65–Q76, 754–756.3) Appendicular
limb / dysmeliahand deformity:Lowerhip:knee:Genu valgum · Genu varum · Genu recurvatum · Discoid meniscus · Congenital patellar dislocation · Congenital knee dislocationfoot deformity:Either / bothdactyly / digit:reduction deficits / limb:multiple joints:Axial Craniofacial dysostosis:other:spinal curvature (Scoliosis) · Klippel-Feil syndrome · Spondylolisthesis · Spina bifida occulta · SacralizationThoracic skeletonribs:sternum:M: JNT
anat(h/c, u, t, l)/phys
noco(arth/defr/back/soft)/cong, sysi/epon, injr
proc, drug(M01C, M4)
Categories:- Congenital disorders of musculoskeletal system
- Greek loanwords
- Deforming dorsopathies
- Vertebral column



Wikimedia Foundation. 2010.